
Presentation
Sudden onset shortness of breath and right sided chest pain.
Patient Data
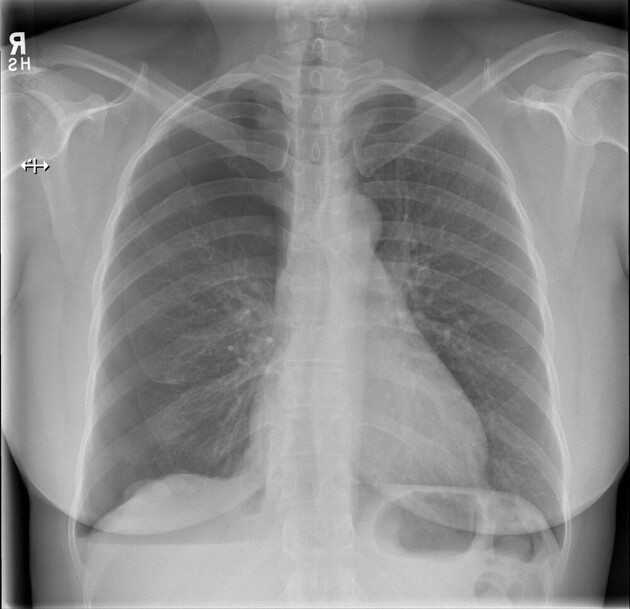
Moderate right sided pneumothorax. Small right-sided pleural effusion. The left lung and pleural space are clear.




Moderate right sided pneumothorax. Overlying the right hemidiaphragm there are large nodular lesions in keeping with endometriosis. The underlying lung shows mild visceral pleural thickening in places and atelectasis due to the pneumothorax. Small right pleural effusion. Triangular shaped nodule, 6mm, within the left lower lobe warrants a follow-up CT.
No enlarged axillary, supraclavicular, mediastinal or hilar lymph nodes. Left thyroid nodule.
Normal heart size and no epicardial coronary artery calcification.
Hepatic and renal cysts, otherwise unremarkable appearances of the visualized non-contrast upper abdominal viscera. The bones are normal.
Conclusion:
Right sided pneumothorax and pleural nodules in keeping with endometriosis.
Case Discussion
This patient presented with a constellation of findings, including spontaneous pneumothorax, dense right basal pleural nodules, a right pleural effusion and on further imaging, bilateral adnexal masses. She was subsequently diagnosed with endometriosis with pleural endometriotic deposits (confirmed at surgery) leading to catamenial pneumothorax.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.