
Presentation
2 days of right lower quadrant pain. 13 weeks pregnant.
Patient Data
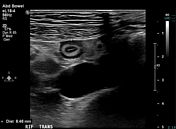
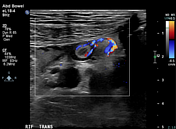

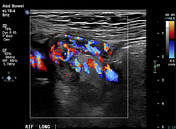
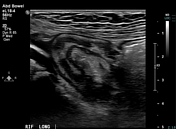
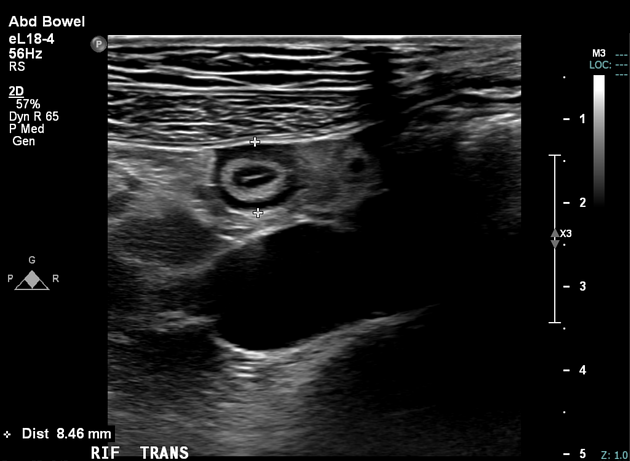
Blind-ending tubular structure identified in the right iliac fossa measures 8.5 mm in diameter (AP) and appears to communicate with the cecum. The structure is highly vascular with trace free fluid along its length and tip (trans, long). The appendiceal target sign is present, with a fluid-filled lumen, hyperechoic inner mucosal layer and hypoechoic outer muscularis layer.
Thin-walled gallbladder without visible gallstones. The imaged maternal kidneys and ovaries appear unremarkable.
Conclusion
Sonographic features are in keeping with acute uncomplicated appendicitis. General surgical review is recommended.

Single live intrauterine gestation with crown-rump length of 66 mm, in-keeping with stated gestational age of 13 weeks by last menstrual period.
The fetal heart rate is 165 bpm.
Case Discussion
This 25-year-old woman presented with 2 days of vague central abdominal pain followed by sharp right lower quadrant pain. She was 13 weeks pregnant (G1P0) and had normal serum inflammatory markers.
Ultrasound of the abdomen revealed acute uncomplicated appendicitis with a healthy fetus. She underwent laparoscopic appendectomy the next day. Intraoperative findings were of an inflamed but not perforated appendix with some purulent fluid in the pelvis. The cecum and appendix were located just inferior to the lower border of the liver.
Histopathology confirmed acute uncomplicated appendicitis. No fecolith was identified. She was discharged home on day 2 post-operatively. Follow-up obstetric ultrasound one month later was unremarkable.
Acute appendicitis remains the most common non-obstetric surgical emergency of pregnancy, with an incidence of up to 0.2% 1. Although fetal mortality is rare in uncomplicated disease, it has been reported as high as 37% in cases of perforation 2. This highlights the importance of prompt diagnosis and treatment in pregnant women.
Ultrasound is the first-line imaging modality of choice for cases of suspected appendicitis in pregnancy given its speed and availability. If non-diagnostic, MRI is the next best choice.
The target sign of acute appendicitis is a subtype of type of the bowel wall target sign and represents mural thickening in the context of acute inflammation. Though usually referenced in the context of CT, it has also been described in abdominal ultrasound 3.
Case courtesy of Dr Simon Li.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.