
Presentation
Known hypertensive, presents with longstanding chest pain and shortness of breath.
Patient Data

Cardiomegaly. The aorta is unfolded. Both costophrenic angles are blunt. There are reticulonodular opacities in both lung fields. Thoracic bony cage is normal.
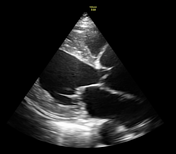



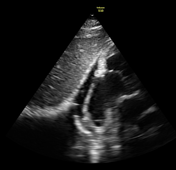


Dilated left ventricle with moderately impaired systolic function (LVEF;30%).
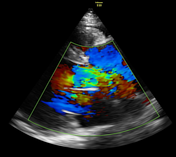
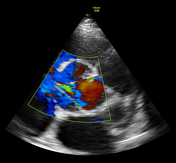
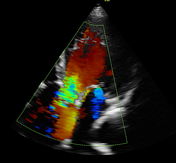
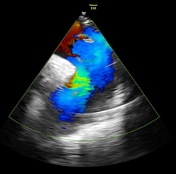
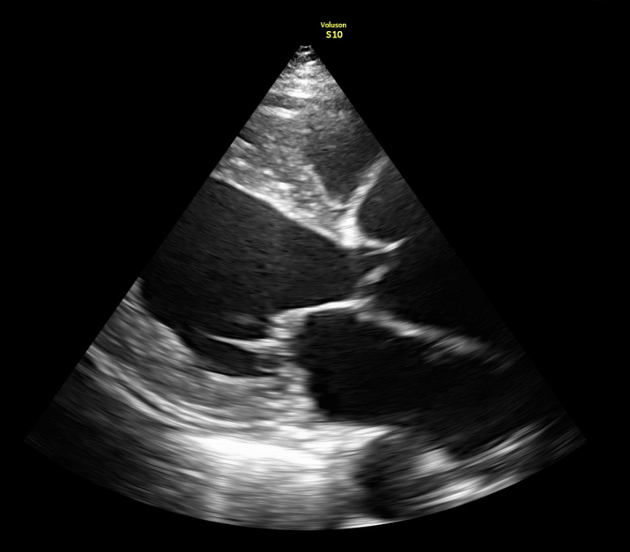
Aortic valve is tri-leaflet. Dilated aortic root, ascending aorta and descending aorta with severe aortic regurgitation. There is an intimal flap distal to the left subclavian artery origin extending downwards as seen on the suprasternal view.
Moderate mitral regurgitation. Mild pericardial effusion.
Case Discussion
This is a typical case of an aortic dissection seen as separation of the aortic intima and media creating a false lumen on the proximal segment of the descending aorta. The above case falls under Stanford classification type B / DeBakey classification type III. Hypertension is one of the most common causes of aortic dissections especially in elderly patients.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.