
Presentation
Sudden onset of persistent pleuritic chest pain, with associated syncope, tachycardia, hypotension and hypoxia.
Patient Data
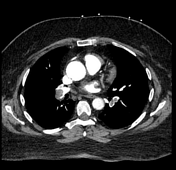


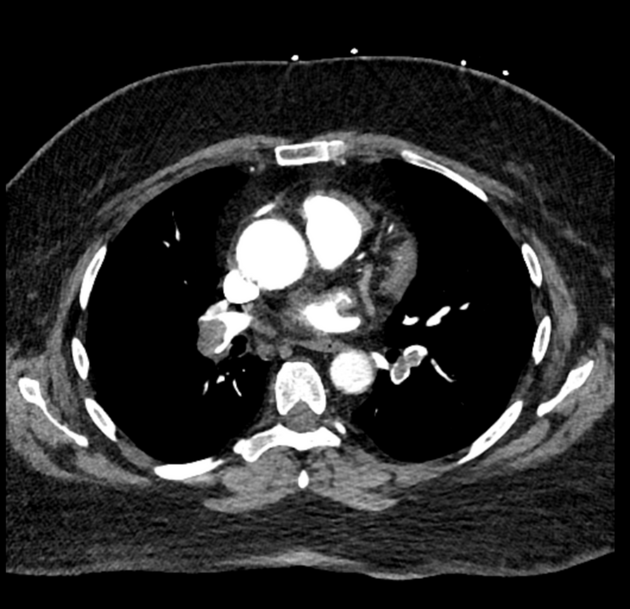
There are large filling defects in both main pulmonary arteries extending into lobar and segmental pulmonary arteries in keeping with bilateral massive pulmonary embolism.
The RV/LV ratio is equal to 1.5, in keeping with right heart strain.
Case Discussion
This patient presented with very classical signs of pulmonary embolism, including shortness of breath, pleuritic chest pain and tachycardia. She had many risk factors for venous thrombosis, including; a locally invasive cholangiocarcinoma, her chemotherapy agents (cisplatin1 + gemcitabine2), and was taking an oral contraceptive.
The patient did not have any calf tenderness, but ultrasound doppler revealed an occlusive thrombus in her right posterior tibial vein. This was likely the source of her pulmonary embolism.
The patient was commenced on therapeutic enoxaparin and was admitted to the intensive care unit for inotropic support. She recovered uneventfully and was stepped down to a direct oral anticoagulant on discharge.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.