
Presentation
Palpatations, right ventricular mass seen on echocardiogram.
Patient Data


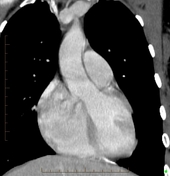


Large heterogenous hyperenhancing mass with a hypoenhancing rim and central stellate scar in the atrioventricular groove, exerting mass effect on the right atrium and ventricle.
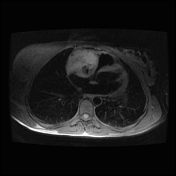
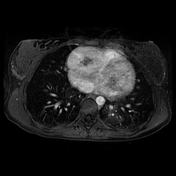
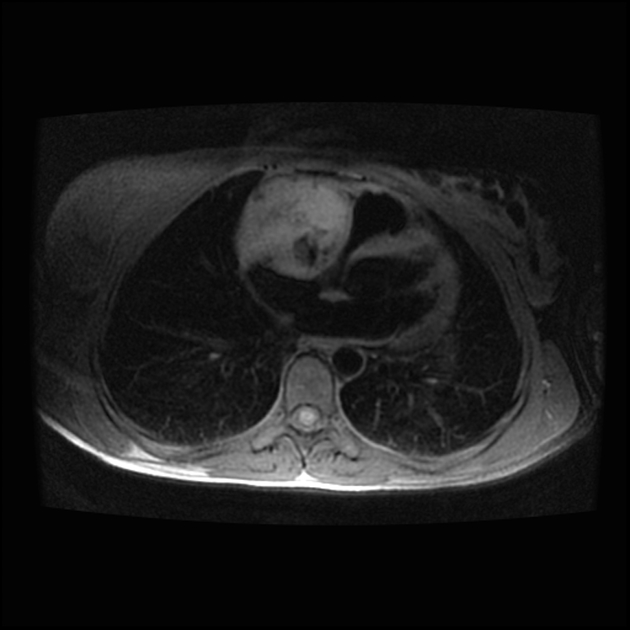
The mass is centered in the atrioventricular groove. It is well circumscribed, demonstrating T1 hyperintensity with internal cystic components, with avid contrast enhancement.
Based on CT and MRI, the initial differential diagnosis consisted of paraganglioma and hemangioma.
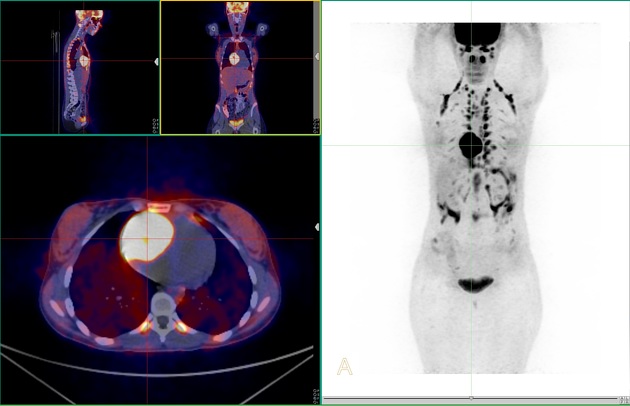
The cardiac lesion demonstrates avid FDG uptake on PET.
There are no other sites of disease.
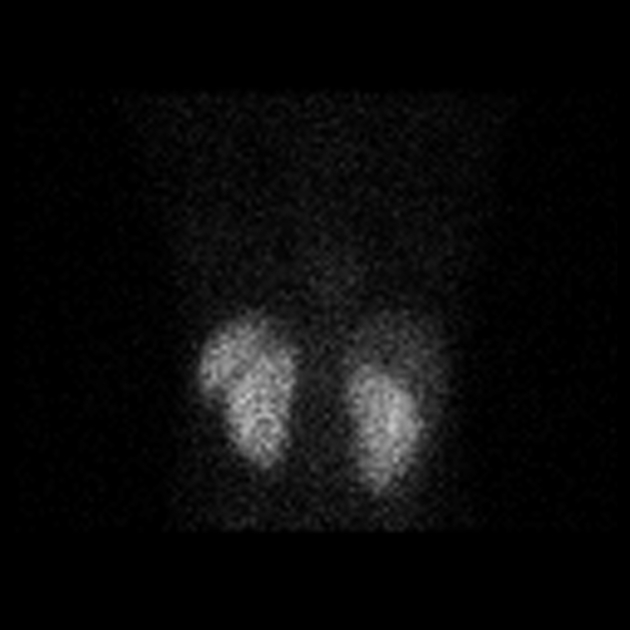
In-111 octreoscan demonstrates the presence of somatostatin receptors.
Case Discussion
The patient's biochemical workup revealed elevated chromogranin A, as well as elevated plasma and 24-hour urine metanephrine. Based on the biochemical profile, radiologic and nuclear scans, paraganglioma was the favored diagnosis.
The patient was referred to cardiac surgery for resection. Intraoperatively, the mass was confirmed to be within the atrioventricular groove. It was successfully resected but required repair of the right ventricle with a bovine pericardial patch and coronary artery bypass of the right coronary artery using a saphenous vein graft.
Histopathologic analysis showed that the tumor had typical features of a paraganglioma with no negative morphological features. Mitoses were not readily identified.
There has been no evidence of radiologic or biochemical recurrence since the surgery.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.