
Presentation
Two month history of retro-ocular headache, rapid visual deterioration and four day history of diplopia
Patient Data
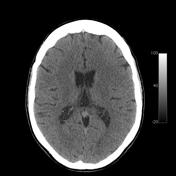

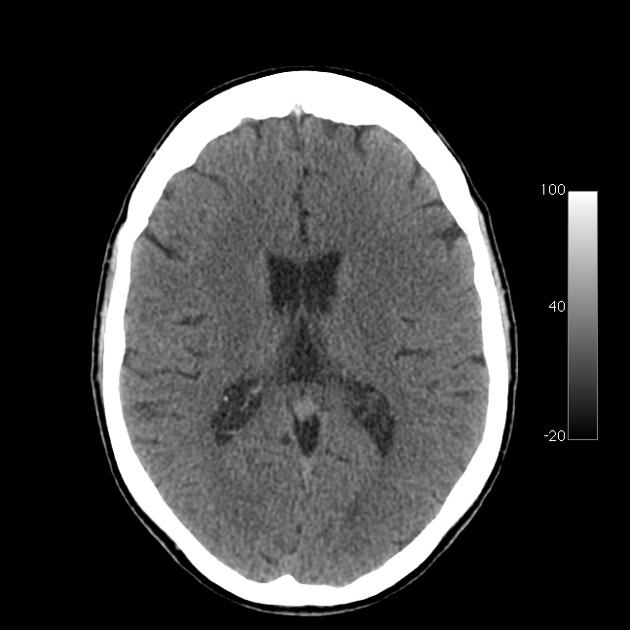
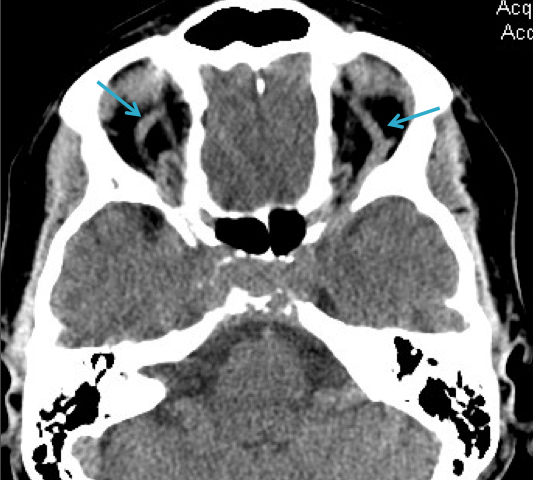
Non-contrast CT of the brain demonstrates no parenchymal abnormality. There is however some increased density within the sella turcica. The superior ophthalmic veins are prominent.
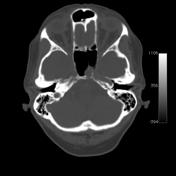
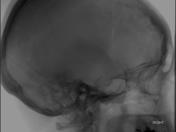
Windowing to bone demonstrates erosion of the sella, with protrusion of soft tissue material into the sphenoid sinus.
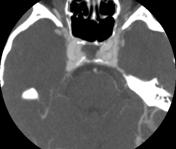

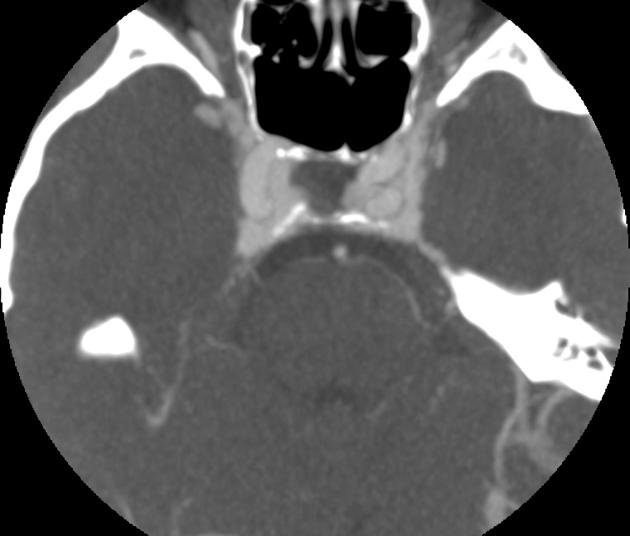
The soft tissue mass seen on non-contrast CT, protruding into sphenoid sinus is demonstrated to be vascular tissue on the CTA of the circle of Willis. The superior ophthalmic veins are markedly enlarged.
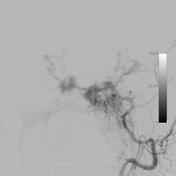
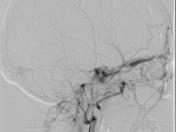
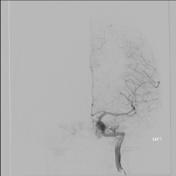
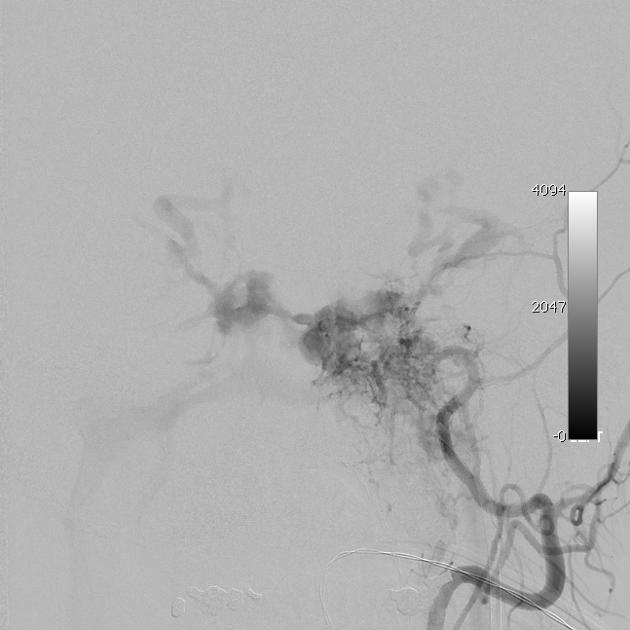
DSA of the left ECA demonstrates early filling of the cavernous sinus with reflux of contrast into bilateral opthalmic veins and inferior petrosal sinuses. A similar pattern was seen following injection of the left ICA, right ECA and to a lesser extent, the left ICA (the latter not included here).
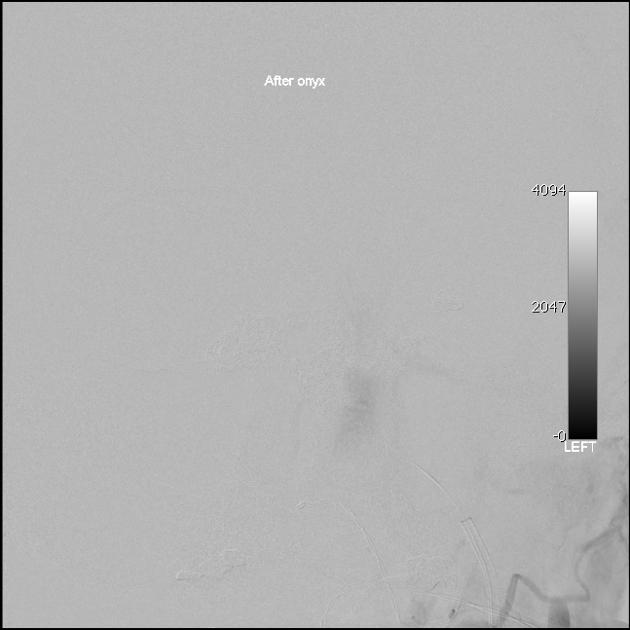
Total occlusion of the fistula was achieved following deployment of coils at the outflow of left superior opthalmic vein and right cavernous sinus, and injection of Onyx.
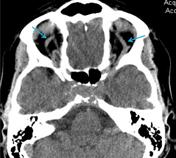
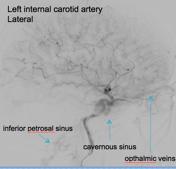
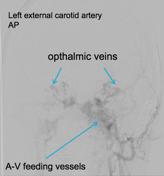
Enlarged opthalmic veins
Case Discussion
This case demonstrates an indirect caroticocavernous fistula with feeders from bilateral ICA and ECAs. Prominence of the superior ophthalmic veins indicative of the increased, retrograde flow was a key diagnostic feature on the CT.
Erosion of the sella by the expanding cavernous sinus in an unusual feature, probably indicating chronicity of this fistula. The fistula was successfully treated angiographically.
A caroticocavernous fistula (CCF) may be due to either a direct connection between the cavernous ICA and the cavernous sinus (and present acutely), or due to an indirect connection via small branches of the ICA, ECA, or as in this case - both. In an indirect CCF, the presentation may be more insidious.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.