
Presentation
Incidental detection of a chiasmatic mass lesion, in the MRI followup after prior resection of posterior fossa pilocytic astrocytoma.
Patient Data


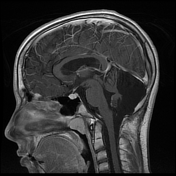
Selected MRI images demonstrating postsurgical changes after remote resection of prior JPA, with no recurrence of the posterior fossa JPA. The chiasmatic lesion did not yet exist. Sequela of left striatocapsular infarct.

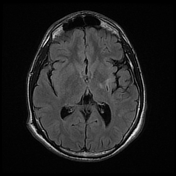
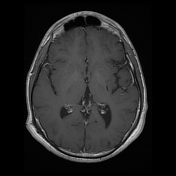
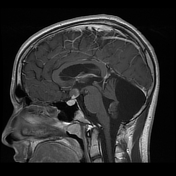
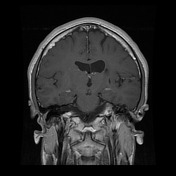
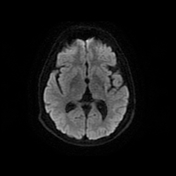
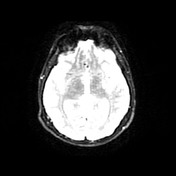
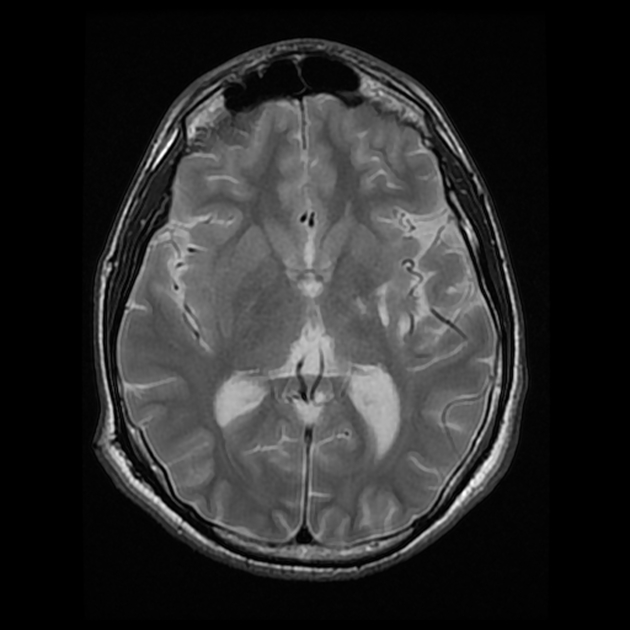
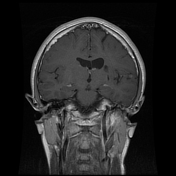
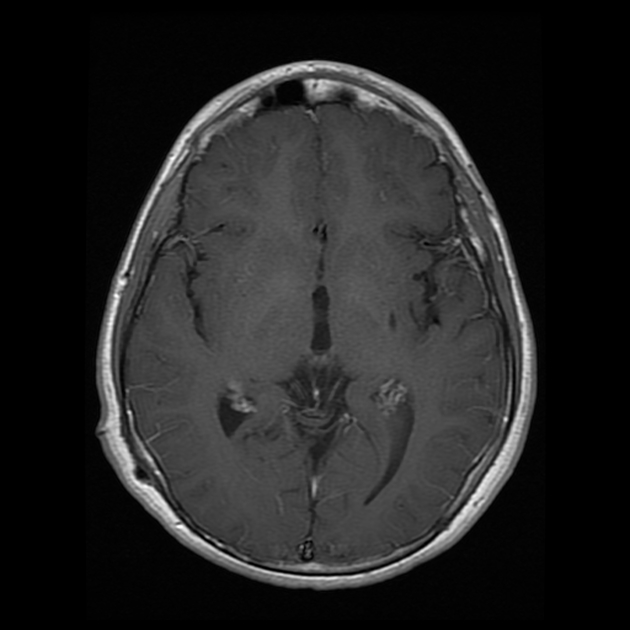
Interval development of chiasmatic mass lesion, containing solid and cystic components with heterogeneous enhancement and mass effect over the hypothalamic region. Again, no recurrence of prior posterior fossa JPA.




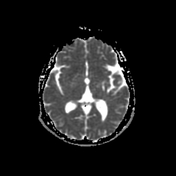
Selected follow up CT images demonstrating continued progression of the optic chiasm mass with further cranial extension, obstruction the foramina of Monro with a transependymal CSF migration in spite of presence of a right transparietal VP shunt.
Case Discussion
The diagnosis of chiasmatic/hypothalamic JPA was histologically proven. There is a left remote striatocapsular infarct, that was present on transfer and the exact cause was unknown.
Key learning point: This case shows a reoccurrence of JPA in a place not related to the primary site and raises the question if this is secondary to prior leptomeningeal dissemination.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.