
Presentation
Diffuse abdominal pain, malaise and generalized body aches for one day. No fever, or respiratory/urinary/bowel symptoms. Known diabetes mellitus, hypertension and morbid obesity.
Patient Data




Fecal loaded colon. No significant bowel dilatation, air-fluid levels or pneumoperitoneum is seen. A few small opacities are seen in the left lumbar region which are likely renal calculi. Osteopenia and degenerative changes are seen in the visualized skeleton.
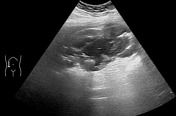

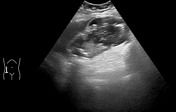


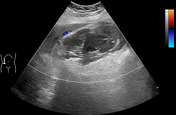

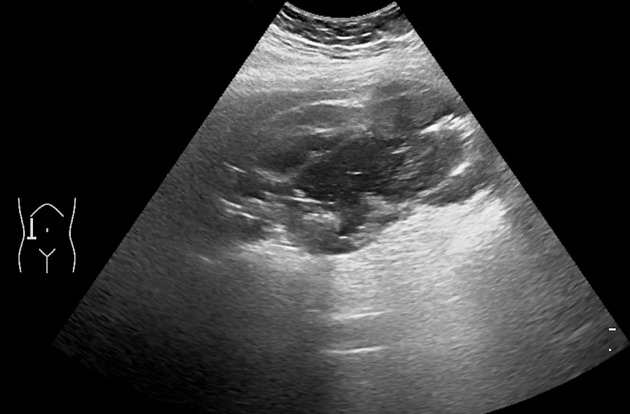
Markedly overdistended gallbladder with heterogeneous appearance and irregular outlines. Maximum diameter of the gallbladder is approximately 8 cm. Multiple small calculi are seen in the gallbladder. Multiple hyperechoic foci suspicious of air are also appreciable within the gallbladder lumen & gallbladder walls. No hyperemia is seen in the gallbladder walls on the color doppler ultrasound examination.
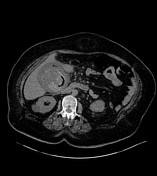



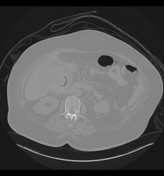
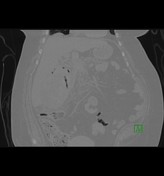
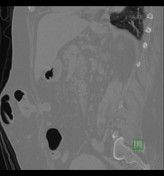


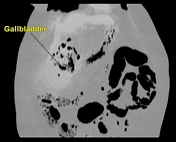

Markedly overdistended gallbladder measuring 8 x 13 cm. Multiple air densities are appreciable within the gallbladder lumen and gallbladder walls. A small radiopaque gallstone is also noted. Some hyperdense contents (density=45HU) are also appreciable within the gallbladder lumen which likely represents inspissated gallbladder secretions or pus. Marked fat stranding is noted around the gallbladder. A few non-obstructive left renal calculi. Supraumbilical anterior abdominal wall hernia containing omental fat and a few bowel loops.
Impression: CT features are suggestive of complicated emphysematous cholecystitis.



Cut surface of the gallbladder showing ischemic changes and diffuse mucosal ulcerations.
Retrieved multiple pigmented gallstones.
Laparoscopic cholecystectomy. Operative findings: Intra-abdominal examination showed gangrenous gallbladder with adhesions to the duodenum and omentum. The gallbladder was perforated and frank pus was coming out from the gallbladder. Approximately 600 ml thick pus was aspirated from the gallbladder. Multiple pigmented stones were also seen in the gallbladder.
Gross pathology
Opened gallbladder measuring 13 cm in length, 9 cm in circumference and 0.8 cm in thickness. There were many perforations seen in the gallbladder wall. The external surface was irregular and brownish. Mucosa was diffusely ulcerated & covered with exudates.
Final pathological diagnosis
Suppurative and gangrenous acute and chronic cholecystitis with diffuse ulceration and pericholecystitis.
Case Discussion
Emphysematous cholecystitis (EC) is an uncommon subdivision of acute cholecystitis. It is a lethal anaerobic infection, associated with a high mortality rate of 15-20% due to high prevalence of complications like gall bladder wall gangrene and perforation 1. In spite of its higher complications and mortality, these patients usually present with nonspecific symptoms, are not critically sick and initially cannot be differentiated from the simple acute cholecystitis 1. Patients with poorly controlled long-standing diabetes may not complain of classical pain in the right hypochondrium due to diabetic neuropathy 1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.