
Presentation
6 months of weight loss and rectal bleeding.
Patient Data
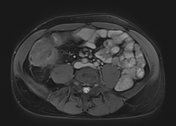



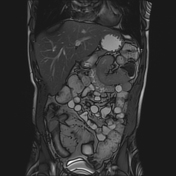
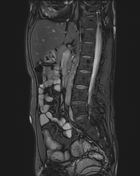
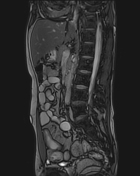
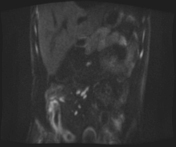
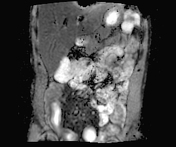
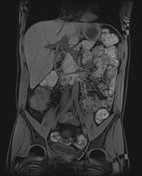

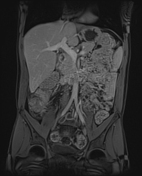
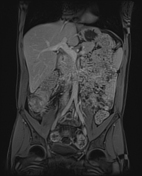
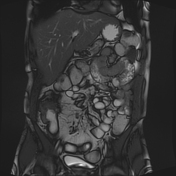

There are signs of active inflammation involving the distal small bowel and proximal large bowel: mural thickening, edema, restricted diffusion and postcontrast hyperenhancement in the distal 30 cm of the small bowel, and the cecum. The enhancement pattern is targetoid, with mucosal and serosal hyperenhancement. Within this abnormal length of the small bowel, there are short segments of sparing, with anti-mesenteric border sacculation in these regions. Upstream from the diseased segment, there is some dilatation. Note also that there is a proliferation of fat within the right lower quadrant, with separation of the diseased bowel loops from the remaining bowel loops within the abdomen. Fistula formation between the ileum and the adjacent cecum can be seen. There are multiple inflammatory lymph nodes in the small bowel mesentery. No disease involvement of the proximal small bowel or the large bowel is identified. There is reduced motility of the inflamed segments of the bowel. There is no free fluid or collection within the abdomen or pelvis.
Case Discussion
At endoscopy, inflammatory changes were noted within the cecum and terminal ileum, with the histological analysis confirming Crohn's disease.
There are classic features of active inflammatory disease, including mural thickening and edema, layering enhancement, restricted diffusion, fat wrapping, and pseudosacculation along the antimesenteric border. In addition, there is transmural disease with fistula formation between the ileum and cecum.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.