
Presentation
Pain.
Patient Data

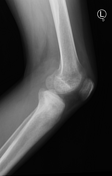
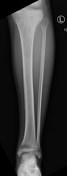


Frontal and lateral views of the left knee and lower leg. There is abnormal sclerosis center on the lateral tibial plateau with an adjacent aggressive appearing periosteal reaction.
Demineralization is present in the distal femur as well as the distal tibia and fibula as well as the talar dome.
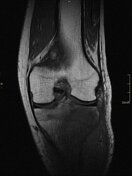

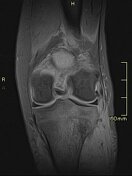
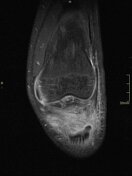
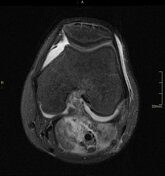


MRI of the knee and lower leg shows:
Ill-defined mass in the lateral aspect of the proximal tibia which extends into the adjacent soft tissues both posteriorly and laterally. The mass measures 7.1 x 5.4 x 8.0 cm (AP by TR by CC). It is T1 hypo intense, T2 hyper intense, and heterogeneously enhancing.
There is an associated suprapatellar joint effusion.
The distal femur, fibular head, patella, distal tibia, and talar dome are unremarkable.



Single phase whole body bone scan performed using 20 mCi of Tc99m MDP IV. Images were acquired approximately 3-hours after radiotracer administration.
There is abnormal intense radiotracer uptake in the proximal tibia corresponding with malignant mass.
There is additional abnormal, but less intense, radiotracer uptake involving the distal femur and about the ankle. These sites were normal on MRI and represent benign reactive osteoblastic activity and/or passive uptake from tumor related left lower extremity hyperemia.
There are no findings concerning for distal bone metastases.
Final Diagnosis
A. Tibial plateau, Left, Biopsy:
· Ewing sarcoma (see comment).
Comment: The morphologic, immunophenotypic, and genetic findings are most consistent with involvement by Ewing sarcoma.
Case Discussion
Ewing sarcoma (ES) is an aggressive small round blue cell malignancy.
Approximately 25% of patients with ES have metastases at diagnosis, most commonly to the lung or other bones.
FDG PET-CT can be optimal for staging Ewing sarcoma; however, a bone scan can occasionally aid in the detection of sclerotic osseous metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.