
Presentation
Work up for epigastric pain, progressive abdominal distention and non-bilious vomiting.
Patient Data
Age: 45 years
Gender: Female
From the case:
Gastric outlet obstruction





Download
Info

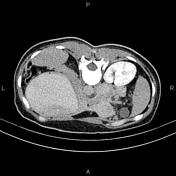
The stomach is over-distended and contrast-filled due to gastric outlet obstruction (GOO). Asymmetrical increased wall thickness is present at the pylorus, accompanied by mild surrounding fat stranding and a few regional enlarged lymph nodes.
Case Discussion
The patient underwent an endoscopy and biopsy, and histopathology evaluation confirmed pyloric adenocarcinoma.
A duodenal or gastric peptic ulcer and then adenocarcinoma are the most common cause of gastric outlet obstruction.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.