
Presentation
Multiple soft tissue swelling on scalp, pyrexia of unknown origin and gait difficulties and painful limp.
Patient Data


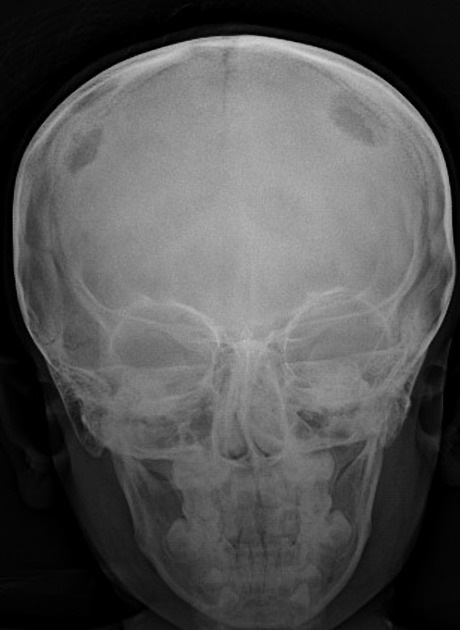
Multiple well defined punched out osteolytic lesions with scalloped edges (geographic skull) are seen in bilateral parital regions. The lesions have a characteristic bevelled edge.
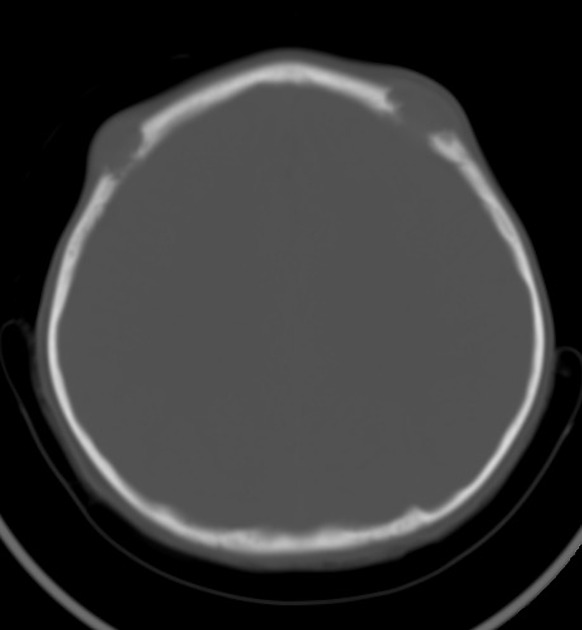
There are multiple osteolytic lesions causing full thickness bone destruction seen in bilateral parietal bones.
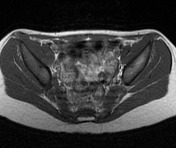


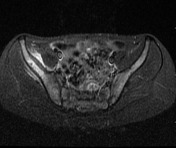
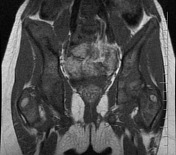
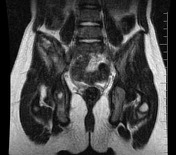
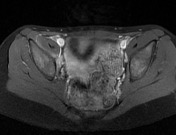

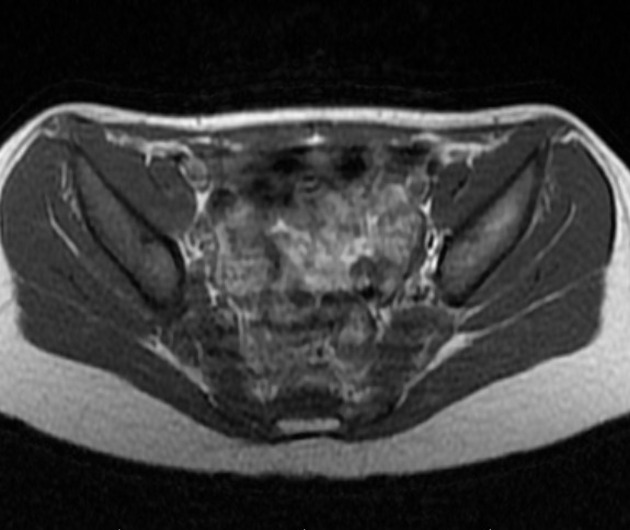
There are abnormal well defined heterogenously enhancing lobulated soft tissue lesions of altered signal intensity along the right iliac blade, bilateral ischium and left femoral diaphysis.. The lesion is causing cortical erosion of the adjacent iliac bone .The lesion appears hypointense on T1W , heterogenously hyperintense on T2 and STIR.
The visualized muscles, bones and rest of the pelvic organs are normal.
The imaging features of the skull, pelvic bones and femoral lesions are most likely suggestive of Langerhans cell histiocytosis
Case Discussion
Histiocytosis X is most often seen in children ages 1 to 15 with the peak incidence at 1-4
years of age.
The rate peaks among children ages 5 to10 years. It most commonly affects skull among the flat bones and femur among the long bones. The diagnostic tests that can be carried out in children are:
- Skin biopsy for the presence of Langerhans cells
- Bone marrow biopsy for the presence of Langerhans cells
- Complete blood count
- X-rays skeletal survey to find out number of affected bones.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.