
The skeleton is the most commonly involved organ system in Langerhans cell histiocytosis (LCH) and is by far the most common location for single-lesion LCH, often referred to as eosinophilic granuloma (EG) (the terms are used interchangeably in this article). For a general discussion of this disease, please refer to the Langerhans cell histiocytosis (LCH) article.
Eosinophilic granuloma accounts for one of the 'Es' in the popular mnemonic for lytic bone lesions FEGNOMASHIC.
On this page:
Epidemiology
The skeletal system is the most common site of Langerhans cell histiocytosis involvement, and in 60-80% of cases, it is the only organ system involved. It primarily occurs in older children and young adults, with a male to female ratio of 2:1.
Clinical presentation
The lesions may be asymptomatic and discovered as an incidental radiographic finding.
When symptomatic, patients complain of pain, swelling and tenderness around the lesion. Systemic symptoms may also be present, including general malaise and, occasionally, fever with leukocytosis.
Pathology
Microscopic appearance
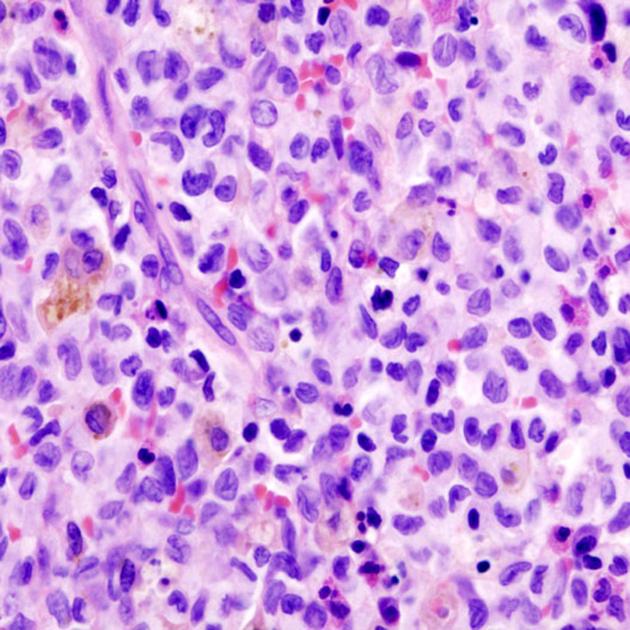
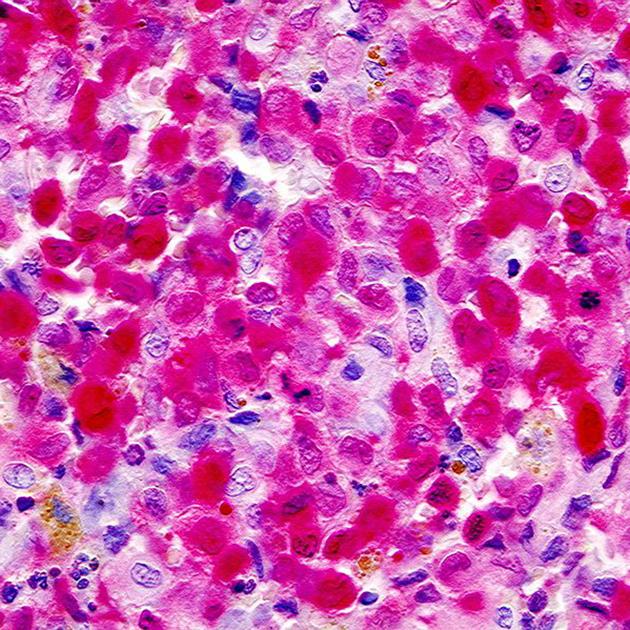
The histologic appearance is characterized by the proliferation of Langerhans cells with an abundance of eosinophils, lymphocytes, plasma cells, and neutrophils. Langerhans cells have a large vacuolated cytoplasm, and vesicular nuclei with linear grooves. Characteristic Birbeck granules, which resemble tennis racquets, are seen by electron microscopy. Langerhans cells produce prostaglandin, which result in medullary bone resorption and this is what causes the symptoms.
IHC staining for CD1a, S-100, and langerin (CD207) are positive 10.
Location/distribution
Patients may have one or, less commonly, many lesions. The most common locations are the skull and long bones 5,6:
skull: ~50%
pelvis: 23%
femur: 17%
spine: ~15% (range 6.5-25%) 7
ribs: 8% (most common in adults)
humerus: 7%
mandible: 7%
Radiographic features
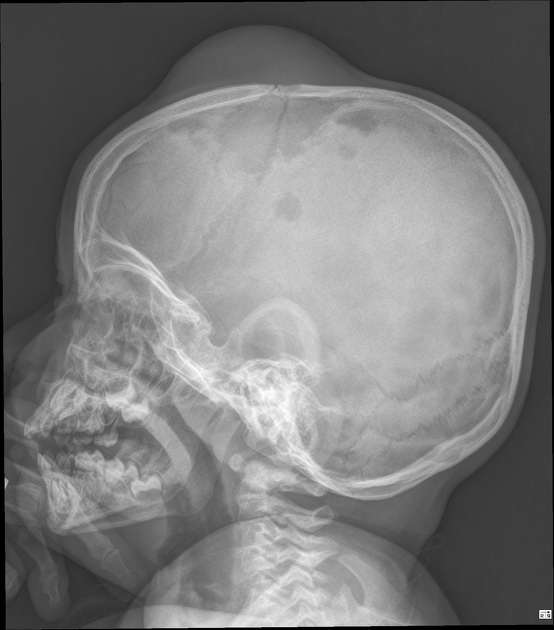
Plain radiograph
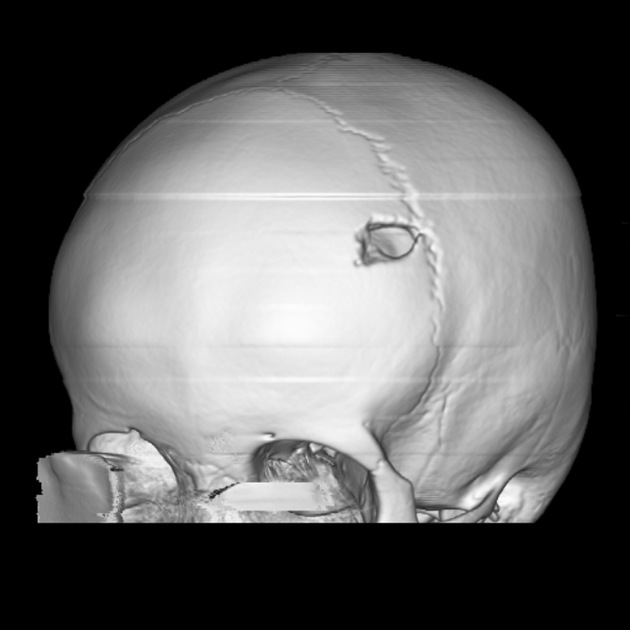
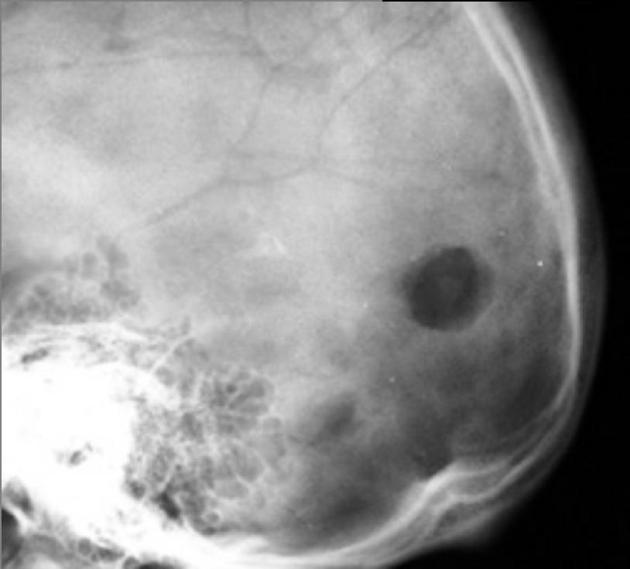
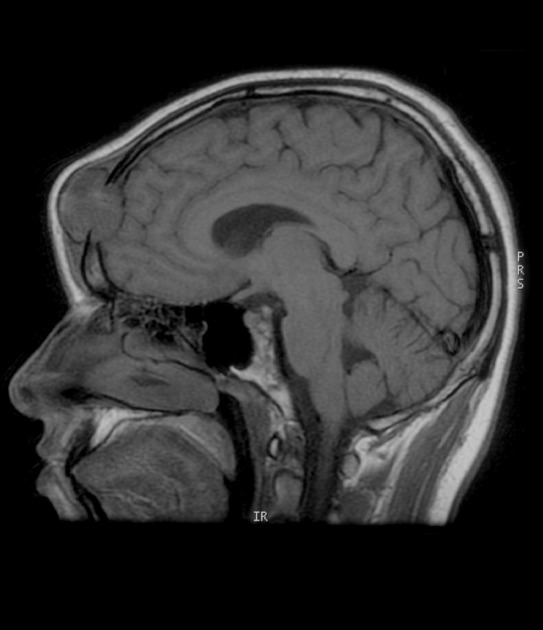
Skull
solitary or multiple punched-out lytic lesions without sclerotic rim
double contour or beveled edge appearance may be seen due to asymmetrical involvement of the inner and outer tables (hole within a hole) sign 8
button sequestrum representing residual bone
Mandible
irregular radiolucent areas mostly involving superficial alveolar bone
floating tooth: loss of lamina dura
Spine
vertebra plana: most common cause of vertebra plana in children; more often in the thoracic spine
Long bones
depends on the phase of disease which is imaged
permeative and aggressive appearing lesion
mainly involves diaphysis or metadiaphysis and respects growth plates
endosteal scalloping, periosteal reaction (in the healing phase it can appear as solid benign periosteal reaction), cortical thinning, intracortical tunneling, and associated soft tissue mass
Ultrasound
Skull
seen as a solid mass lesion
minimal vascularity
originating from the diploic surface, extending through to the outer table
local subperiosteal spread
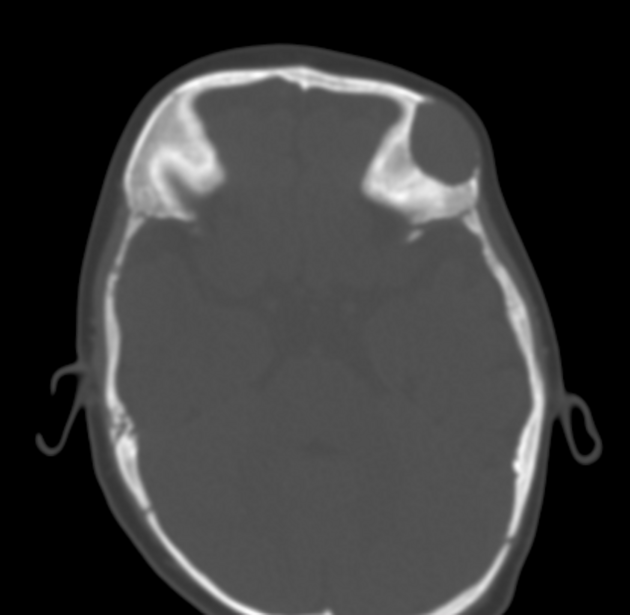
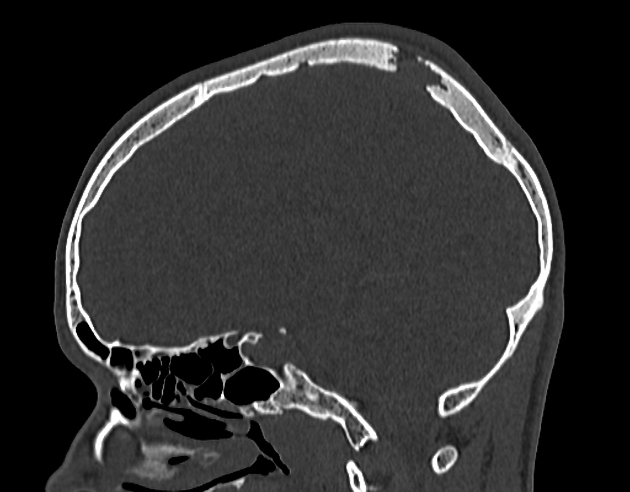
CT
Similar to plain film findings with better demonstration of cortical erosion and soft tissue involvement. Excellent for biopsy and surgical planning.
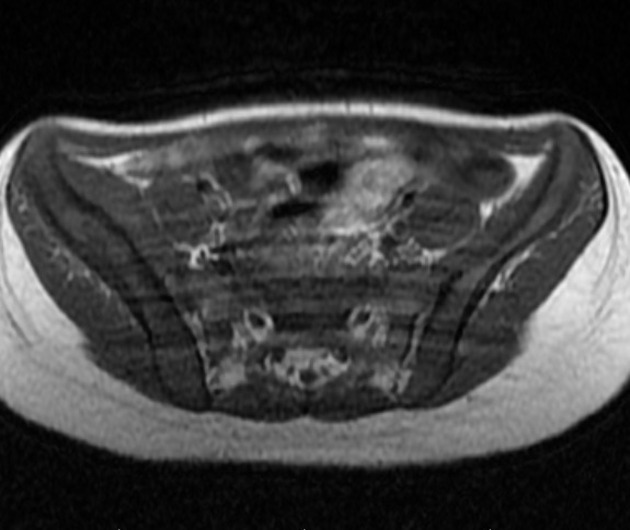
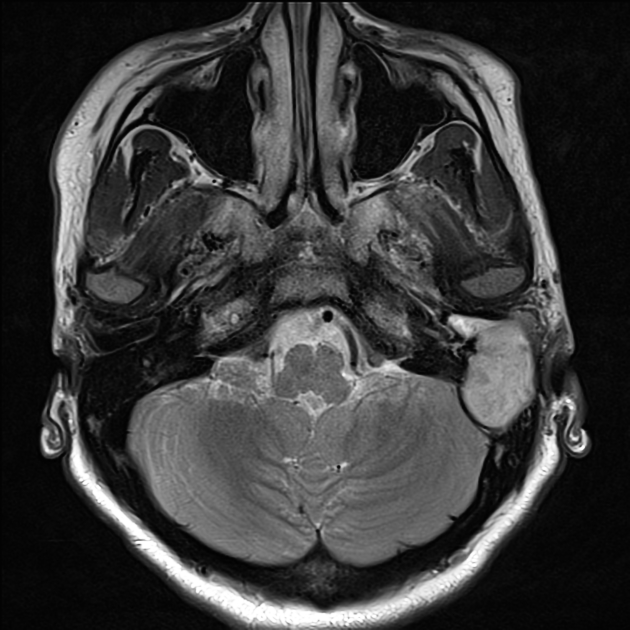
MRI
Signal characteristics include:
T1: typically hypointense to isointense 9
T2: hyperintense 9
STIR: hyperintense
T1 C+ (Gd): often shows diffuse contrast enhancement
Nuclear medicine
Depending on the histological picture, there is a variable appearance on bone scintigraphy, with lesions showing an increased or decreased tracer uptake. Nonetheless, bone scans are helpful in other asymptomatic lesions.
Treatment and prognosis
Prognosis is excellent when disease is confined to the skeleton, especially if it is a solitary lesion, with the majority of such lesions spontaneously resolving by fibrosis within 1-2 years. However, where symptoms persist, other treatment options may be considered:
excision and curettage 3
steroid therapy: intralesional injection
chemotherapy
radiofrequency ablation 4
radiotherapy for spinal lesion
History and etymology
The term eosinophilic granuloma was coined by Lichtenstein and Jaffe in 1940 2.
Differential diagnosis
General imaging differential considerations include:






















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.