
Presentation
10 day history of progressively worsening epigastric pain, abdominal distension, vomiting, constipation and an isolated episode of melena. Previous history of laparoscopic gastric band insertion 7 years prior, known to be eroded 3 years earlier but lost to surgical follow up. Recent increased NSAID use.
Patient Data



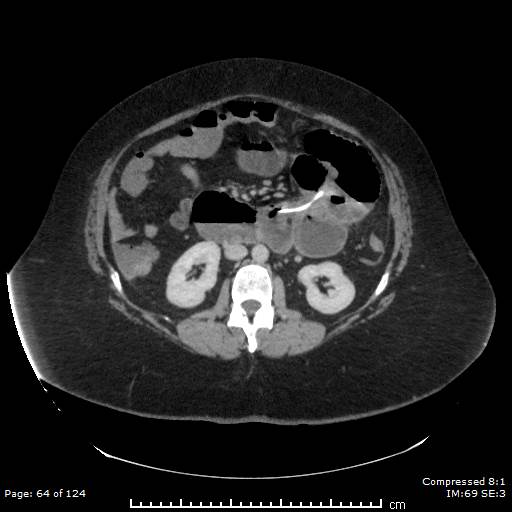
The lap banding device is situated at the level of the illiac crests. It is located within the small bowel loop and appears to be associated with a point where there is a change in caliber of bowel loops suggesting this is causing a proximal obstruction. The tubing extending to the device appears to pass through the lumen of the small bowel loops proximal to this and then through the gastric lumen before extending to its external port. There is irregularity in the wall of the stomach fundus presumably related to change associated with the site of a previous rupture. Additionally, a small well defined collection is detected in the right paracolic gutter.
Case Discussion
This case demonstrates typical features of a small bowel obstruction secondary to a migrated and eroded laparoscopic gastric band, confirmed on CT.
The patient underwent an emergent laparoscopic mobilization and removal of the migrated gastric band located within the jejunum. Post operatively this was complicated by a failed and ulcerated primary anastomosis site due to localized ulceration and perforation. A 10cm small bowel resection and partial gastrectomy was subsequently performed.
The histopathology report confirmed segments of proximal small bowel, consistent with the jejunum and showing transmural perforation with areas of ischemia, hemorrhage and fibrinopurulent exudate around the edges and an abundance of necroinflammatory debris with the bases containing severely inflamed granulation tissue.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.