
Presentation
Sore throat and fever. Anterior neck tenderness. 2 weeks post COVID infection. Concern of tracheitis and retropharyngeal abscess.
Patient Data


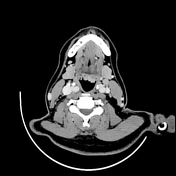


Enlarged, hyperenhancing lingual tonsil extending into the vallecula and depressing the epiglottis. Irregular mucosal surface with no associated collection. Mild stranding within the pre-epiglottic fat. Asymmetric edema of the aryepilottic folds (left greater than right), trace prevertebral edema and multiple prevertebral lymph nodes. Overall, the changes result in mild narrowing of the hypopharynx and supraglottic airway. No narrowing of the glottis and subglottic airway.
Asymmetric inflammatory fat stranding extending into the anterior neck around the sternohyoid and sternocleidomastoid muscles. Cervical chain lymph nodes are prominent bilaterally with surrounding fat stranding.
Mucosal thickening and secretions throughout the imaged paranasal sinuses. The mastoid air cells and middle ear cavities are clear. The partially imaged intracranial structures are unremarkable. No acute fracture or suspicious osseous lesion demonstrated. The lung apices are clear.
Impression
Enlarged lingual tonsil with up moderate surrounding inflammatory change. The appearances are suspicious for lingual tonsillitis, with the differential including lymphoid hyperplasia and malignancy. No associated collection.
Associated depression of the uvula and mild supraglottic airway edema, with mild reduction in airway diameter.
Case Discussion
The patient was negative for EBV, RSV, influenza A and B and settled well with symptom relief. The presumed diagnosis was COVID tonsillitis which has been reported in the literature.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.