
Presentation
Presented to neurology OPD of the hospital with complaints of low back ache with pain radiating to both the lower limbs since 2 years aggravated in last 1 week associated with new onset bladder incontinence.
Patient Data
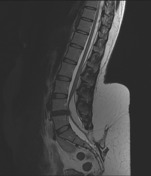



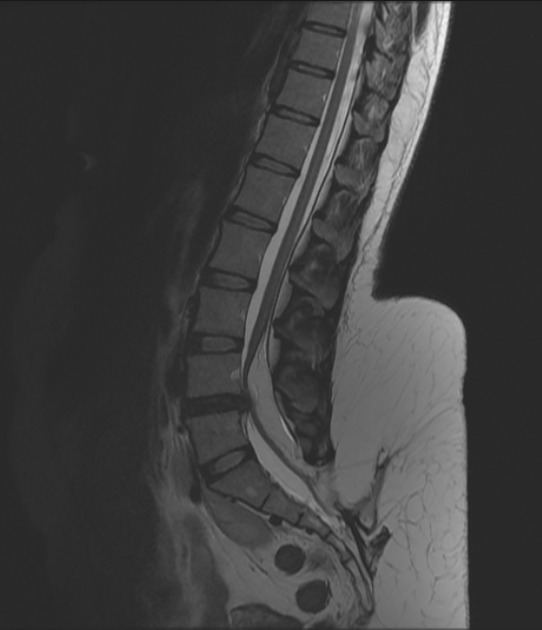
Low lying cord noted at L4 with fatty mass dorsal to cord displacing the cord ventrally with lipoma-placode interface within the spinal canal with normal anterior subarachnoid space.
The lipoma is contiguous with subcutaneous fat through dorsal dural defect at level of S2 vertebral body ( spina bifida ). These features are diagnostic of Lipomyelocele.
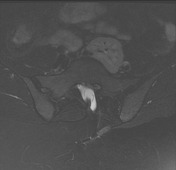
Also noted is ectopic left kidney seen in the pelvis.
Case Discussion
Lipomyelocele (LMC) is one of the commonest closed spinal dysraphism presenting as subcutaneous mass. It is seen in thoracolumbar region and usually presents as fatty subcutaneous mass. It is twice as common as lipomyelomeningocele (LMMC) as against open spinal dysraphism wherein myelomeningocele is more common than myelocele.
As the spinal canal grows, there is distortion of nerve roots with growth; thereby leading to neurological deficits highlighting the importance of early diagnosis.
Posterior spinal defect noted which is covered with skin and shows interspersed lipomatous tissue.
The neural placode-lipoma interface lies within the spinal canal or at its edge with normal anterior subarachnoid space.
There is usually associated tethered low lying cord or syrinx of terminal spinal cord.
Spinal dysraphisms are associated with congenital renal anomalies.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.