
Presentation
Hypertension and cardiac arrhythmias. Prior surgery.
Patient Data




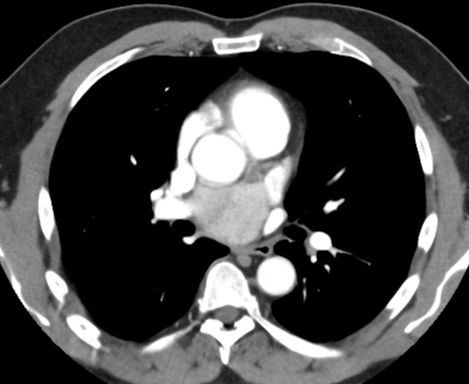
Marked heterogeneous enhancement of a 5 x 4 cm mass which lies posterior to the ascending aorta and between the right pulmonary artery and left atrium in the visceral compartment of the mediastinum.
Surgical clips at the posterior margin.
Elevated noradrenalin, dopamine and serotonin secretion were attributed to the tumor.
Alpha and beta blockade was instituted prior to biopsy.
Surgical excision was attempted elsewhere but abandoned because of adhesion to vital structures.
Surgical excision subsequently performed on cardiopulmonary bypass with cardioplegia and necessitated removal of portions of the aorta, pulmonary artery and left atrium.
Left atrium opened, LA roof excised with tumor and reconstructed with bovine pericardium (3x6cm).
Diagnostic summary:
1. Paraganglioma: Paraganglioma, 55mm, mitotic activity low with 1 mitosis note per more than 20 HPF, Ki67, approximately 1%, SDHB deficient/loss.
2. Posterior left atrium: Negative for malignancy.
3. Left superior pulmonary vent: Negative for malignancy.
4. LA roof: Negative for malignancy.
Microscopic Description: Specimen 1: Paraganglioma. The sections show a partially encapsulated and relatively well circumscribed tumor composed of small nests ("zell ballen") and small sheets of large epithelioid cells with plentiful slightly granular cytoplasm and predominately central rounded nuclei. Scattered cells have markedly enlarged nuclei. Chromatin ranges from fine granular to more coarse and vesicular. The small nests in many areas appear surrounded by a layer S100 positive sustentacular cells. There is diffuse positive staining for CD56, chromogranin and synaptophysin. The lesion invades ("mushrooms") through the partial capsule into the surrounding adipose tissue. There is no necrosis and lymphovascular space invasion is not seen. Mitotic activity is infrequent with only 1 mitosis noted in greater than 2 square millimeters of tumor. The Ki67 proliferation rate, although heterogeneous, is in the order of 1%. The immunoperoxidase study for SDHB shows absence of staining of the lesional cells. The lesion focally appears to abut the circumferential margin of the specimen, possibly separated from the inked surface by only a single strand of collagen in some areas (eg Blocks 1B, 1F and 1K). The features are consistent with a paraganglioma.
Case Discussion
Paragangliomas are rare tumors in the mediastinum and are more common in the visceral compartment. They usually present in adults due to compression of adjacent structures or secretion of catecholamines. Biopsy and surgery are hazardous due to hemorrhage, hypertensive crisis and involvement of adjacent vital structures 1.
Incomplete excision may lead to local recurrence. Alpha and beta blockade is important to avoid hypertensive crisis precipitated by biopsy or surgery. Finally, they are often syndromic and associated with succinate dehydrogenase mutations. In this case, there was 1% SDHB deficiency or loss.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.