
Presentation
Confusional state and right hemiparesis.
Patient Data



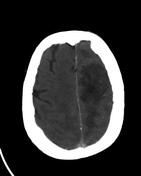
No radiographic sign of an acute infarct.
The arteries of the neck (not shown) and head are patent, with no stenosis.
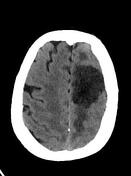
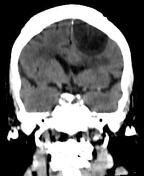
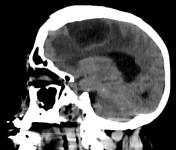
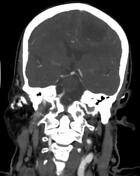
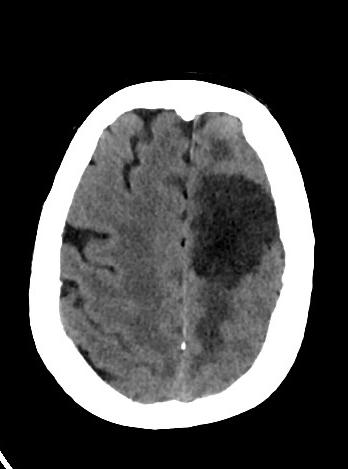
Left frontal hypodense non-enhancing (necrotic? cystic?) extra-axial mass measuring 3.7 x 5.3 x 3.9 cm (TRV x AP x CC), with rim enhancement. Perifocal vasogenic edema. Mass effect expressed as extensive sulcal effacement, deformation of the left ventricle, and minimal subfalcine herniation.
Left occipital nodule lateral to the occipital horn of the left ventricle, with focus of calcification - cavernoma most probably.
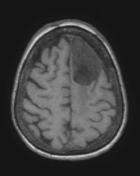
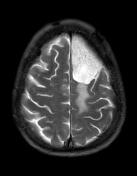
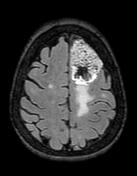



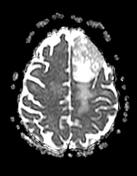
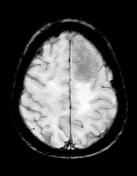
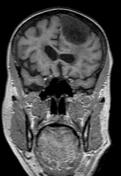

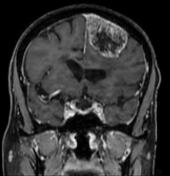
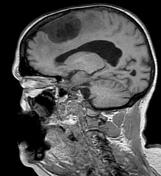
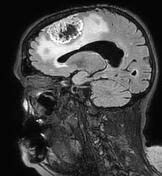
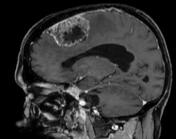
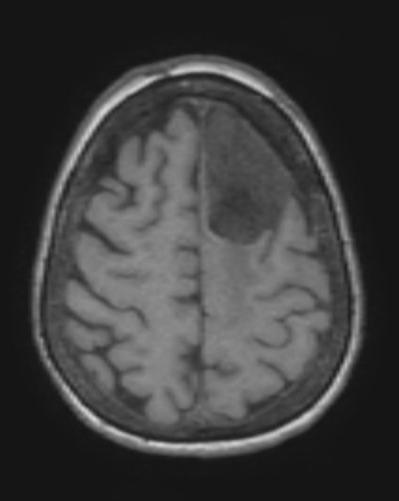
Large left frontal extra-axial mass containing innumerable tiny cysts, with intensely enhancing solid component (i.e. the rim and in-between the cysts). Intratumoral hypointense area on FLAIR, T1, and contrast-enhanced T1, perhaps representing necrosis. Subtle dural tail. Extensive perifocal edema with mass effect mostly on the left ventricle.
Left occipital susceptibility focus, most probably representing a cavernoma.
On the fluid-sensitive sequences, hyperintense periventricular and subcortical white matter changes represent substantial microangiopathy.
Case Discussion
She went on to have a craniotomy, with the removal of a meningioma.
Histopathology report:
Meningioma, CNS WHO grade 1.
The tumor shows microcystic change.
Immunostains: the tumor cells are positive for EMA, PR; negative for ER markers; supporting the diagnosis.
Microcystic meningioma is a rare meningioma variant which leads to atypical imaging appearances.The microcysts represent extracellular spaces, scattered throughout the meningioma substrate. These tumors usually also show abundant vascularity. On both CT and MRI, the imaging appearances are dominated by the high water content of these tumors, with characteristic very high T2 signal as in this case.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.