
Presentation
Incidental finding during work-up and treatment for acute appendicitis.
Patient Data
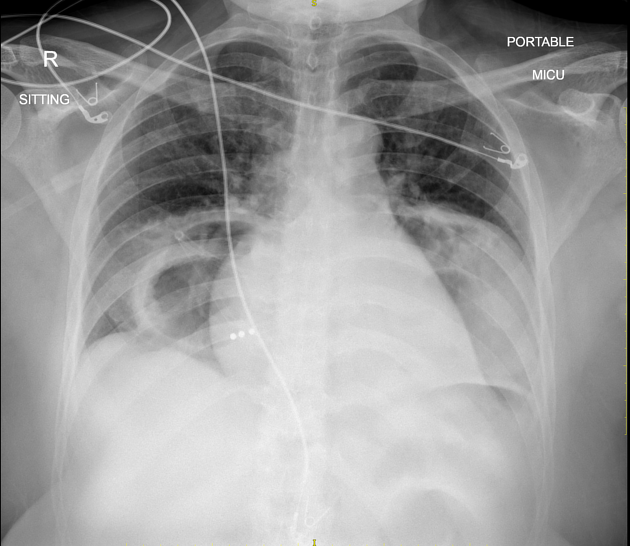
The portable post-appendectomy X-ray confirms a nasogastric tube in situ with the distal tip supra-diaphragmatic and projecting overlying the right heart border. The proximal portion of the tube is poorly appreciated, however, it does not appear to be endotracheal or endobronchial in origin.
There is a somewhat symmetric, curvilinear, mixed-density mid to lower zonal appearance. There are no overt features to suggest a diaphragmatic rupture on plain film.
Free left subdiaphragmatic intraperitoneal air is a normal post-appendectomy finding.
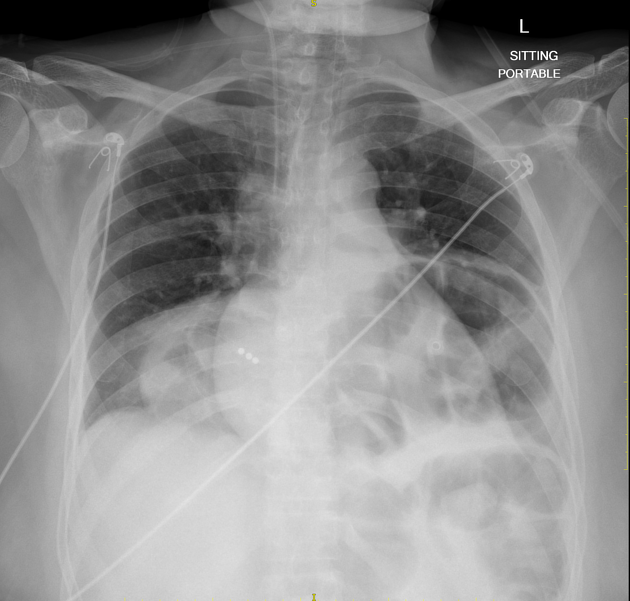
Day 2 imaging demonstrates a supradiaphragmatic large bowel loop, with the nasogastric tube tip, right of the midline and supradiaphragmatic too.




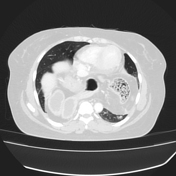
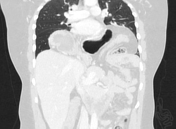
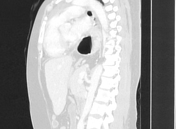
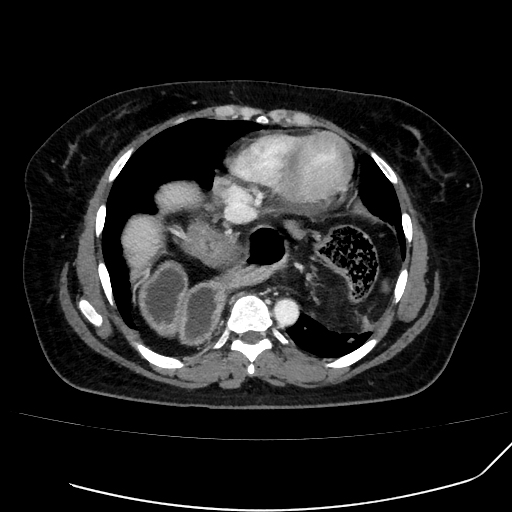
The pre-appendectomy CT study confirms a compound or mixed para oesophagal hiatal hernia (type 4). There is complete gastric herniation with an abnormal rotation, however no gastric outlet obstruction and hence no gastric volvulus. There is herniated mesenteric fat, with small and
large bowel. There is adjacent atelectasis as expected. There is no diaphragmatic rupture.
There is peri splenic-free fluid in a setting of complicated acute appendicitis.
Case Discussion
A case of a compound hiatal hernia in an asymptomatic patient who presented with complicated acute appendicitis and underwent emergency appendectomy. Although the stomach appeared fluid-filled, there was the noted absence of vomiting and epigastric pain which affirmed the CT suspicion of gastric rotation rather than a gastric volvulus.
The chest X-rays over 2 days demonstrated intermittent large and small bowel herniation through the large esophageal hiatal diaphragmatic defect giving rise to the unusual chest X-ray appearance.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.