
Presentation
Stable angina, history of posterior wall infarction with "an occluded coronary artery" long ago.
Patient Data




Technique
patient premedication: beta blocker and nitrates
acquisition method: step and shoot (prospective acquisition)
contrast injection protocol: triphasic injection
standard image reconstruction
Findings
normal coronary origins and proximal courses
balanced coronary arterial dominance
corkscrew-like tortuous terminal vessels
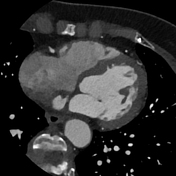
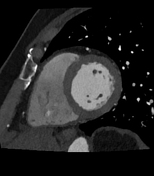
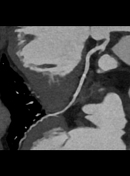
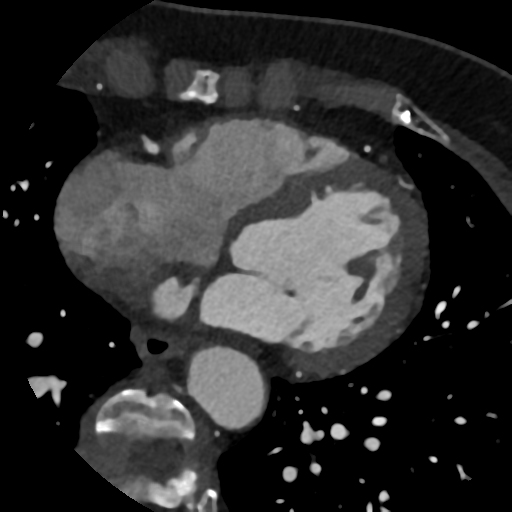
circumscribed myocardial thinning and narrow subendocardial hypoperfusion of the midventricular inferior segment
Plaque burden:
calcium score (according to Agatson, not shown): 0
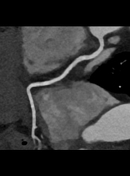
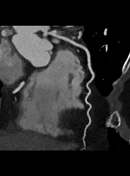
Right coronary artery (RCA): gives rise to posterior descending artery (PDA)
no plaques or stenoses in the proximal, middle and distal segments
posterior descending artery with abrupt caliber reduction and filiform distal vessel
Left main: inconspicuous
Left anterior descending artery (LAD): one diagonal branch, septal branches
no plaques or stenoses in the proximal, middle and distal segments
no plaques or stenoses of the diagonal branch
Circumflex artery (Cx): three obtuse marginal branches, posterolateral branch
no plaques or stenoses in the main epicardial vessel
no plaques or stenosis of the marginal and posterolateral branches
Impression
status post inferior wall infarction with circumscribed myocardial scarring of the inferior wall probably as a result of an occlusion of the posterior descending artery
otherwise no coronary plaques or stenosis
corkscrew-like tortuous terminal vessels indicating hypertensive disease
Exam courtesy: Yvonne Kühn (radiographer)
Case Discussion
A coronary CTA with a circumscribed myocardial scar of the midventricular inferior wall in a patient with a previous myocardial infarction, probably due to an occlusion of the posterior descending artery and otherwise inconspicuous coronary arteries. Further digging into the patient's medical history revealed that the occlusion was known and revascularization was not an option in the past due to distal location and the small size of the vessel. Therefore, optimization of medical therapy was recommended.
The past medical history and the visible indentation of the myocardium aid in the evaluation of this case, where one should be careful not to take it as an inconspicuous examination. Unfortunately, the patient could not yet be persuaded to have a cardiac MRI for better visualization of her myocardial scar.
Courtesy: Dr Waltraud Ibe


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.