
Presentation
Neck crepitus and chest pain. Two days post dilation for GEJ stricture due to Barretts esophagitis.
Patient Data


Oral and IV contrast CT.
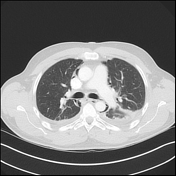
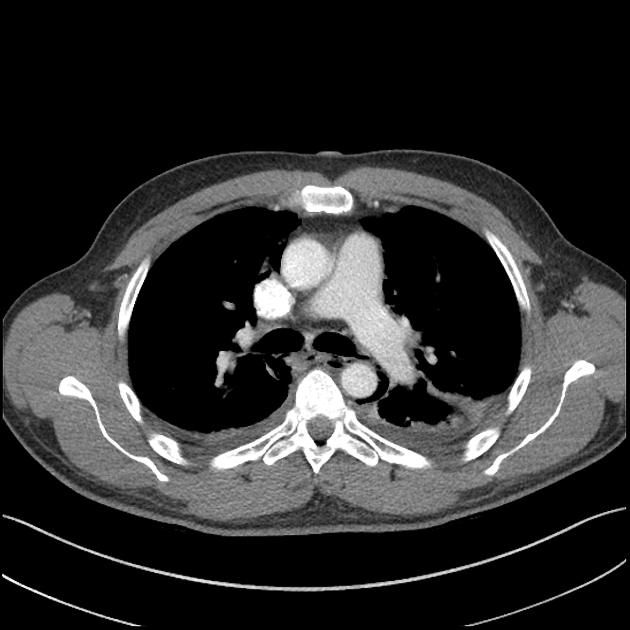
Extensive pneumomediastinum and surgical emphysema in the subcutaneous tissues and prevertebral soft tissues of the neck. No evidence of pneumopericardium.
Contrast extravasation from the distal thoracic esophagus, to the left and posteriorly at the level of T8. Left para-esophageal posterior mediastinal collection at the level of the perforation.
Air space opacification of the right lower lobe with volume loss, in keeping with right lower lobar collapse. Near complete airspace opacification of the left lower lobe. Fluid in the left major fissure. Bilateral pleural effusions.
Fluid density right midpole renal cyst. The imaged portion of the liver, spleen, pancreas, gallbladder and adrenals and stomach have a normal appearance. No concerning osseous lesion.
IMPRESSION
Perforated distal thoracic esophagus (at the level of T8) with pneumomediastinum and surgical emphysema in the prevertebral and subcutaneous tissues of the neck.
Bilateral pleural effusions. Right lower lobar collapse. Airspace opacification in the basal left lower lobe.
Case Discussion
The patient was taken to theater and a left posterolateral thoracotomy performed through the 7th ICS. The collection contained pus and a 1cm anterolateral esophageal defect was located and repaired. A temporary feeding jejunostomy was also performed.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.