
Presentation
Sudden onset headache.
Patient Data
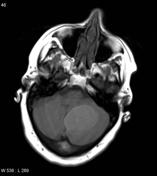


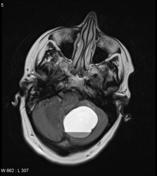
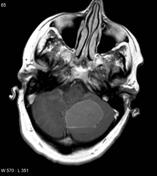
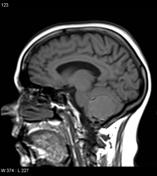
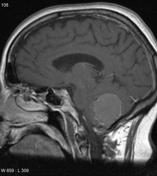
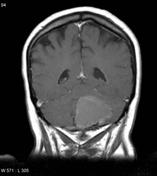
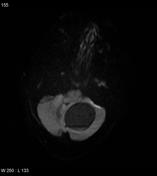
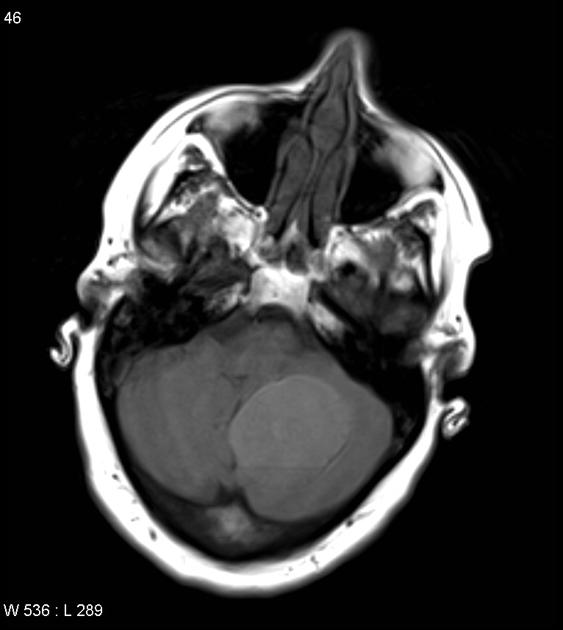
There is a large cystic lesion in the posterior fossa, to the left of the midline. It has a fluid fluid level and does not attenuate on FLAIR. Intrinsic high T1 signal and peripheral hemosiderin is in keeping with blood produces. Inferiorly, a number of nodules are present which do not however demonstrate clear contrast enhancement. There are no abnormal flow voids.
Case Discussion
In a young adult, the differential for a cystic lesion in the posterior fossa is really between a pilocytic astrocytoma and a hemangioblastoma. The absence of flow voids favors the former. Both lesions can uncommonly hemorrhage.
The patient went on to have a resection.
Pathology
MICROSCOPIC DESCRIPTION: The sections show cerebellar tissue containing tumor with greatly variable appearances. The cerebellar tissue itself is atrophic, with marked gliosis. The tumor contains areas of organizing old hemorrhage and extensive areas of calcification, including a large calcified nodule as described macroscopically. Calcification appears to relate to proliferated, small, thick-walled blood vessels. There are areas of proliferation of piloid astrocytes, with fine elongated cytoplasm and fairly regular oval nuclei, with scattered granular bodies and Rosenthal fibers evident. In places there is a well developed fascicular architecture. Neither mitotic figures nor microvascular proliferation are apparent.
FINAL DIAGNOSIS: Pilocytic astrocytoma, WHO grade 1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.