
Presentation
Day 2 post MBA. Abdominal pain and SOB. Desaturation. Altered mentation.
Patient Data
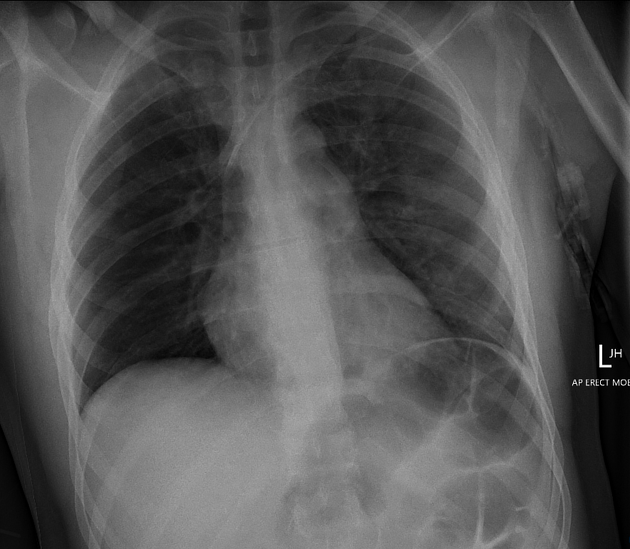
Left-sided subclavian CVL projected within the SVC.
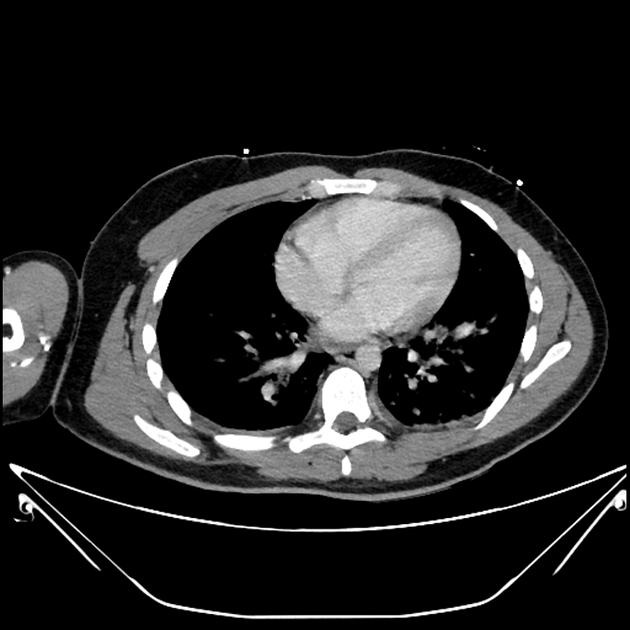
Ground-glass opacification within both lung apices and the left lung, better delineated on prior CT chest in keeping with suspected fat embolism. No pneumothorax or pleural effusion. Cardiomediastinal contours are within normal limits. Right clavicle fracture. Dilated large bowel loops within the left upper abdomen.
Initial trauma CT 2 days prior
Multiple fat density filling defects in the proximal right femoral vein. The largest deposit at the junction of the external iliac/femoral vein anterior to the right femoral head. Displaced right proximal femoral fracture. Fracture haematoma and oedema expands the anterior and medial compartments of the right upper thigh.
Relatively small volume IVC. No evidence of filling defect in the IVC or of the right ventricle.
Diffuse low attenuation of the liver consistent with steatosis. Spleen, adrenals, pancreas and kidneys appear normal. Vicarious excretion of contrast layering within the gallbladder. IDC in the bladder. Incidental midgut malrotation.
Case Discussion
The patient had pulmonary fat embolism syndrome secondary to the right femoral fracture.
Acute decrease in GCS was investigated with CT head which was normal (as were several other CT heads over the next 2 weeks). A brain MRI was never performed.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.