
Presentation
Headache. Recurrent vomiting for 1 week, Recent occipital craniotomy 3 weeks ago for surgical resection of right cerebellar tumor.
Patient Data
Age: 4 years
Gender: Male
From the case:
Pseudomeningocele



Download
Info

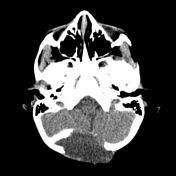
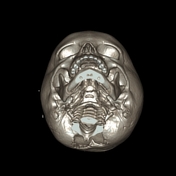
- subcutaneous/subgaleal bilocular CSF collection at the back of the head and upper nape overlying occipital craniotomy defect, with possible communication with cisterna magna (pseudomeningocele)
- left frontoparietal subdural fluid collection (hygroma/chronic hematoma) with underlying mass effect, mild rightward midline shift, attenuation of the left lateral ventricle and mild dilatation of the right lateral ventricle (subfalcine herniation)
- infra-tentorial right posterior fossa subdural fluid collection (hygroma)
- right cerebellar hemisphere posterior cortical and subcortical area of encephalomalacia
Case Discussion
Right cerebellar pilocytic astrocytoma was first discovered on MRI performed 1 month ago, which was operated on and the patient had an uneventful post-op period of 2 weeks, after which another MRI was done and revealed subdural hygromas/chronic hematomas, right cerebellar encephalomalacia and pseudomeningocele.
One week later, the patient started developing recurrent vomiting, for which non-contrast CT brain was requested. Upon the diagnosis of subfalcine herniation, urgent neurosurgical consultation was advised and the patient was submitted for surgery.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.