
Presentation
Pleuritic chest pain. Dry cough.
Patient Data





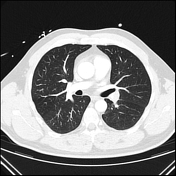
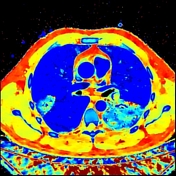

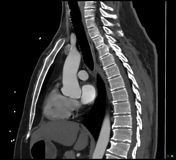
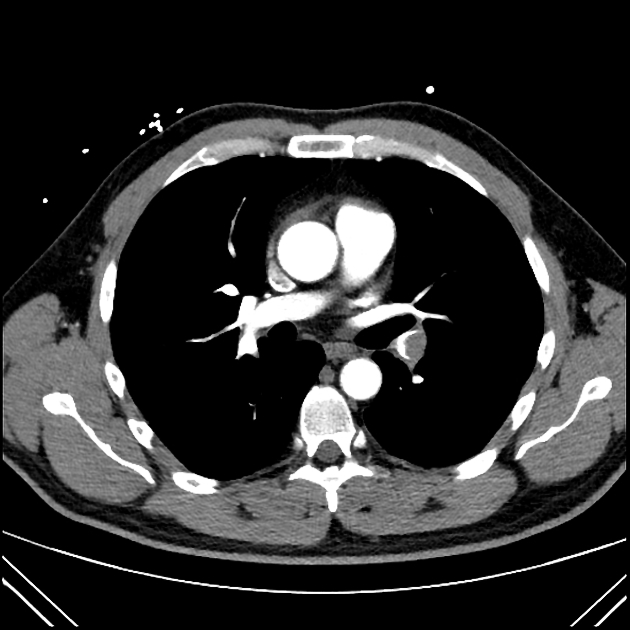
The scan is of good diagnostic quality. Pulmonary embolus at the origin of the left lower lobar pulmonary artery extending into its segmental branches, with associated reduced perfusion on the spectral images. Further occlusive emboli in the medial segment of the right middle lobe and a subsegmental artery in the posterior segment of the right upper lobe, again with perfusion changes on the spectral images. Non-occlusive embolus in the right lower lobe. No CT evidence of right ventricular strain. RV/LV ratio is 0.9 (normal is <1.0). The heart and mediastinal structures are normal.
Patchy ground glass change in the left lower lobe, most confluent in the left costophrenic angle, which may represent developing changes of infarct in this setting. No pneumothorax. Small left pleural effusion
The upper abdominal viscera are unremarkable. No mass in the lower neck. Bones and soft tissues are normal.
IMPRESSION
Study positive for PE, with large embolism at the origin of the left lower lobe pulmonary artery extending distally, and smaller emboli in the right lung.
Case Discussion
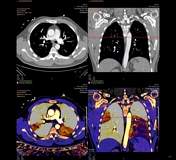
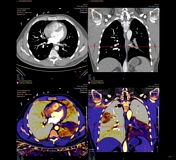
Case example of positive CTPA with a dual-layer spectral CT:
- the low monoenergetic (monoE, 45 keV) recons are used to provide an iodine boost to the pulmonary arteries, good if there is suboptimal contrast opacification.
- the Z effective (Zeff) recons provides a map of perfusion which details the presence of contrast in the lung, good to identify perfusion defects that may be due to subtle PEs.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.