
Presentation
History of metastatic melanoma.
Patient Data


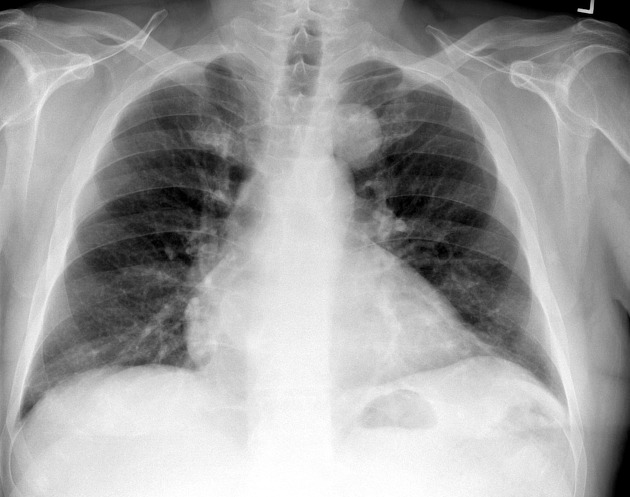
There is a round ~4 cm left suprahilar opacity projecting superior and slightly lateral to the aortic knob on PA view. It overlaps the middle compartment mediastinum. There may be higher-density components of internal calcification.
Close scrutiny of overlapping tissues shows that the lesion is separate from the aorta and left paratracheal stripe, most consistent with a mass centered in the pulmonary parenchyma.
Recommend CT for further evaluation.




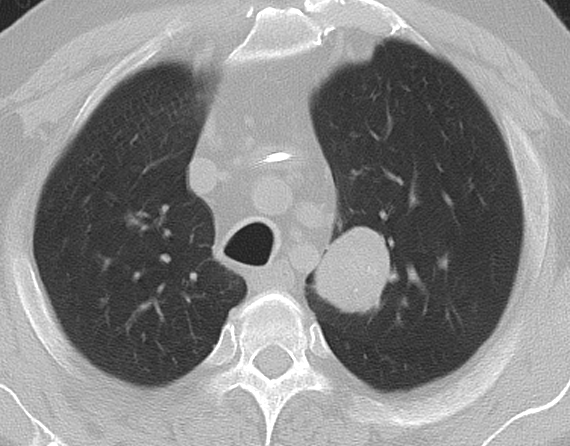
A 4 cm mass within the apical segment left upper lobe contains bulky calcifications, soft tissue density, as well as a smaller amount of low-density consistent with bulk fat content. This lesion corresponds to the findings on radiograph.
These findings are most consistent with a benign hamartoma.



A follow-up evaluation shows no interval change in appearance of the left upper lobe mass with calcification and fat components, again most consistent with benign hamartoma.
ROI drawn at the inferior aspect of the lesion shows density consistent with fat.
Case Discussion
Given the patient's history of aggressive malignancy, the finding on the initial chest radiograph is suspicious and warrants further evaluation by CT imaging.
The finding of bulk fat within a pulmonary nodule is consistent with a benign etiology, most commonly pulmonary hamartoma or lipoid pneumonia. No follow-up was recommended for this lesion.
A repeat chest CT performed one year later for different reasons shows no interval change in the lesion, again consistent with benign hamartoma.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.