
Presentation
6 month follow-up of incidental lung opacities found on an otherwise normal CT pulmonary angiogram.
Patient Data




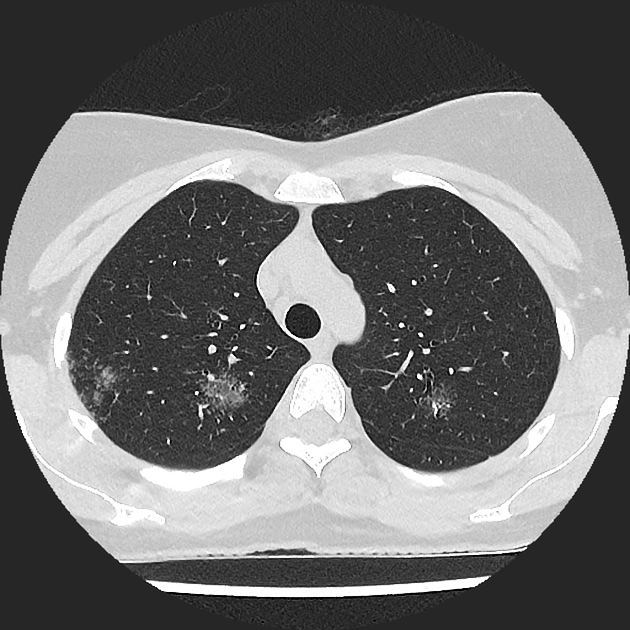
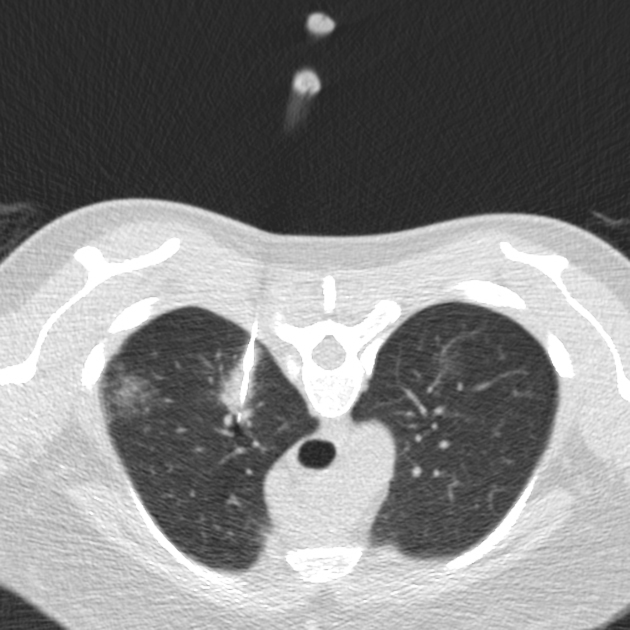
Multifocal rounded ground-glass attenuation opacities with upper zone predominance. Some are bronchocentric and some abut the pleura and fissures. One lesion is associated with retraction of the adjacent fissure.
The granular appearance, clustering and satellite micronodules favor a diagnosis of sarcoidosis. The differential diagnosis could include multifocal adenocarcinoma or organizing pneumonia.
No lymphadenopathy.
No interval change over 6 months.
18G core biopsies had a granular appearance. Important to avoid the oblique fissure and pulmonary blood vessels.
Histology:
The core biopsies of pulmonary parenchyma and airway wall tissue show "innumerable" well-formed, non-necrotizing, granulomata composed of tight aggregates of epithelioid histiocytes and multinucleated giant cells within airway wall tissue (lamina propria and submucosa), alveolar walls and possible septa. Air-space granulomata are not noted. Small numbers of lymphocytes are present within and surrounding the granulomata but there is no acute neutrophilic inflammation and eosinophils are inconspicuous. No refractile foreign material is identified. There is no significant airspace inflammation. Features of organizing pneumonia are not noted. Special stains (DiPAS and Methanamine silver) do not show fungi. The Gram stain for bacteria is negative The Putt stain for acid-fast bacilli is negative. There is no evidence of malignancy. The histological features are those of granulomatous inflammation. The appearances and distribution of the granulomata are consistent with sarcoid. Infection should be excluded by correlation with microbiological studies.
Microbiology negative.
Case Discussion
Pulmonary sarcoidosis - stage 3 (with no hilar lymphadenopathy) accounts for about 10% of thoracic sarcoid.
Distribution (peribronchovascular, subpleural and upper zone predominant), galaxy sign, granular appearance and stability are helpful features.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.