
Ruptured renal angiomyolipoma causing pleuritic chest pain diagnosed on CTPA
Presentation
Left-sided pleuritic chest pain, tachycardia, elevated D-dimer, and taking OCPs. Rule out pulmonary embolism.
Patient Data


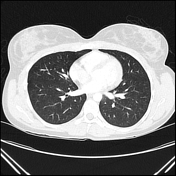
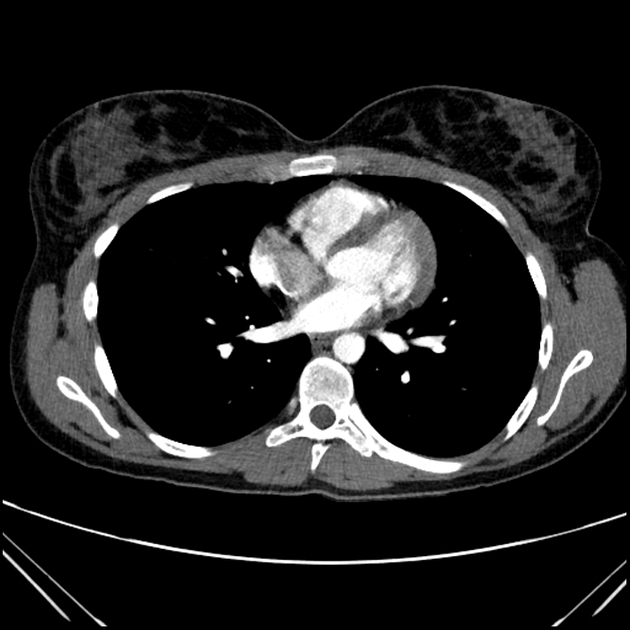
No pulmonary arterial filling defect was identified in a good-quality CTPA. No right ventricular strain. The heart is normal with no pericardial effusion. Normal opacification and caliber of the thoracic aorta. No mediastinal lymphadenopathy.
The lungs are clear. No pleural effusion or pneumothorax.
Moderate left perinephric and subsplenic fluid with density of 28 HU extending around the pancreatic tail. Bulky appearance of the left kidney with focal cortical hypoenhancement of the anterior aspect. Left renal exophytic partially imaged rounded mass approximately 4 cm in diameter arising from the upper pole. No arterial contrast extravasation evident.
No fracture or destructive osseous lesions.
Impression
No PE identified to the level of the subsegmental arteries.
Left retroperitoneal hemorrhage centered on an exophytic (partially imaged) rounded mass arising from the upper pole of the left kidney. No arterial contrast extravasation evident. DDx included tumor (AML, RCC) and abscess complicated with hemorrhage. CT abdomen is advised.
CT abdomen

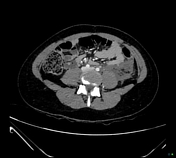



A heterogenous rounded exophytic mass 4 cm in diameter arises from the upper pole of the left kidney. No contrast extravasation. Small foci of intralesional fat. The left renal artery and vein opacify normally. Dense retroperitoneal fluid with a density of 75 HU extending to the intraperitoneal cavity around the spleen and into the left paracolic gutter. Radiodense contrast from the prior scan within the bilateral renal calyces, proximal ureters, and bladder. The right kidney is normal.
The liver, gallbladder, pancreas, spleen, and adrenal glands are normal. No pneumoperitoneum. Normal caliber enhancement of the large and small bowel loops. Prominent, mesenteric lymph nodes, likely reactive.
The lung bases are clear. No suspicious osseous lesions.
Impression
Heterogenous left renal mass with retroperitoneal hemorrhage. The lesion contains macroscopic fat which makes an angiomyolipoma (AML) the most likely diagnosis. When this large, they have a propensity to bleed. Discussion with IR recommended regarding angioembolisation.
Angioembolisation
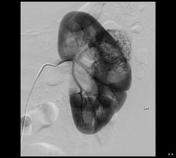
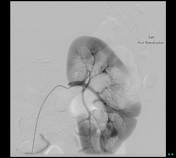
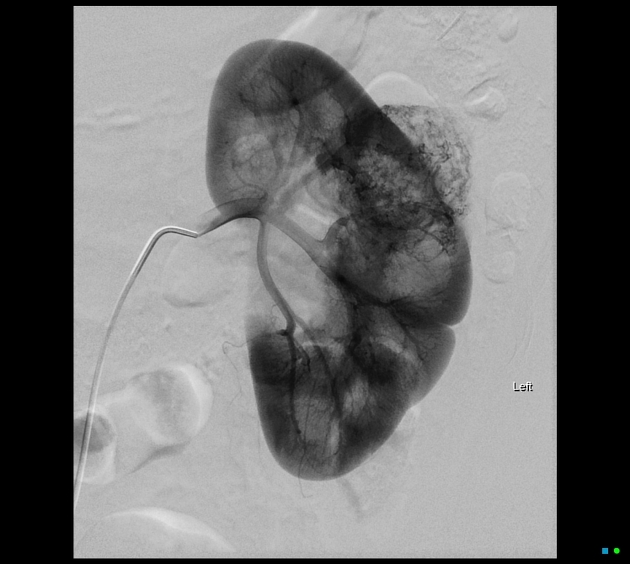
Angiograms demonstrated a 42mm rounded hypervascular lesion with arterial supply from a midpole anterior segmental artery. Gentle embolization with calibrated contour PVA 350-550 micrometer particles.
Satisfactory cessation of feeding arterial flow on completion angiography. Preserved renal cortical enhancement to the renal parenchyma. No significant supply from the posterior division artery.
Case Discussion
The patient recovered well. An MRI several weeks later confirmed the diagnosis of AML. The patient undergoes regular MRI follow-up of the AML.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.