
Presentation
Painless, irreducible umbilical hernia (approximately 7 × 10 cm). The hernia is indurated on palpation, with no detectable bowel sounds. The overlying skin appears necrotic.
Patient Data
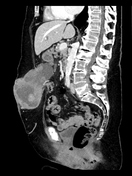





Small hiatal hernia of the distended stomach.
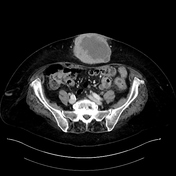
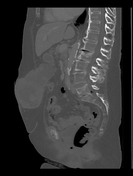
The stomach is in contact with a mass that extends beyond the rectus abdominis muscle and infiltrates the abdominal wall with no clear delineation from the cutis.
The mass shows inhomogeneous contrast enhancement with dilated vessels within the subcutaneous fat of the abdominal wall.
Increased number and suspicious enlargement of mesenteric lymph nodes.
Fibrofatty proliferation is observed in the adjacent adipose tissue.
Histology report
The excision specimen from the abdominal wall tumor in the umbilical region consisted entirely of tumor tissue from a poorly differentiated adenocarcinoma. Based on morphology and immunohistochemistry, the findings were most consistent with an abdominal wall metastasis of previously diagnosed endometrial carcinoma, specifically of the serous subtype. Molecular pathology identified it as a p53-mutated type with positive L1CAM expression, classifying it within a poor prognostic group. HER2 expression was also positive.
Gastrointestinal endoscopy
Esophago-gastro-duodenoscopy revealed type C gastritis but was otherwise unremarkable. Colonoscopy identified a suspicious polypoid mass in the cecum. Histology confirmed a tubulovillous adenoma with low-grade dysplasia and no evidence of invasive growth.
Cancer conference
During the cancer conference, a decision was made to proceed with palliative chemotherapy.
Case Discussion
Differential diagnosis of umbilical masses should comprise hernias as well as neoplasia. For the latter, metastases are more frequent than primary tumors of the umbilicus and may arise from different sites of origin 2. Based on the contact of the mass with the stomach, a gastrointestinal stromal tumor should be part of the differential diagnoses in this patient.
Eight years earlier, the patient underwent hysteroscopic excision for uterine fibroids, of which one was subsequently diagnosed histologically as a 2 mm serous endometrial carcinoma. Laparoscopically-assisted hysterectomy and adnexectomy exposed histological confirmation of pT1a endometrial cancer without nodal or distant metastasis.
Previous CT scans conducted during the follow-up of the patient’s MGUS failed to thoroughly evaluate the abdominal wall mass. In a meta-analysis comprising 336 patients, Gabriele R et al. reported that 15% of umbilical metastases were misdiagnosed as umbilical hernia 2. This case highlights the critical importance of including the search for external hernias in the radiologist’s diagnostic approach. Furthermore, it emphasizes the need for meticulous assessment of the hernia’s contents.
The specific pathomechanism behind umbilical metastasis remains unclear. Yet hypothesis include direct extension, lymphogenic and hematogenic spread 1. The present diagnosis was further complicated by the fact, that the patient was earlier diagnosed with an endometrial carcinoma in situ which had been curatively resected. Cell seeding during surgery as well as coincident endometriosis in an atypical location can be discussed as the origin of recurrence in this patient.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.