
Presentation
Known with chronic asthma. The patient presents with acute, severe, chest pain. There is a confirmed absence of any trauma.
Patient Data

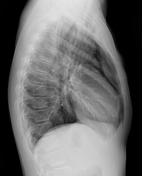

The lung fields are hyperinflated with evidence of a spontaneous pneumomediastinum. Prominent broncho vascular markings are consistent with a history of asthma. There is lower cervical surgical emphysema. The CXR is otherwise unremarkable.
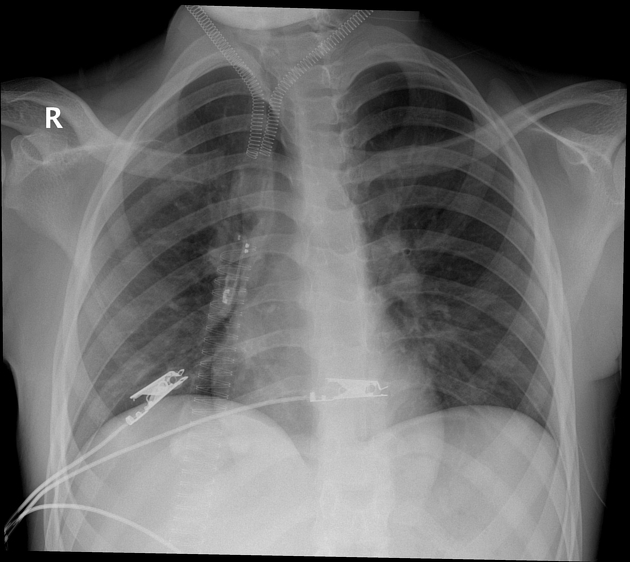
This is a follow-up mobile X-ray. There is an overlying oxygen mask, (likely a Venturi mask) with an unusually armoured appearance mimicking ECMO-type cannulae.
There is a rotated position at the time of exposure.
The surgical emphysema is resolved and there is poor delineation of the pneumomediastinum.
There are overlying ECG
Case Discussion
A case of a spontaneous pneumomediastinum in a young asthmatic. The CT chest was normal except for the pneumomediastium and surgical emphysema as per the initial chest X-ray. There was no obvious source of the pneumomediastium identified.
The armoured oxygen mask may easily mimic ECMO cannulae in a quick cursory review, however on closer inspection one realizes that the metallic coiling is related to the mask or mask strapping around the neck!
The patient recovered without any further incident and was discharged after 4 days in hospital.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.