
Presentation
Abdominal pain.
Patient Data

Mildly distended small bowel loops with air-fluid levels.
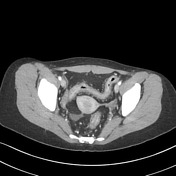



Diffuse colonic wall thickening from the rectum to the cecum, with fat submucosal deposition seen in the rectum (fat halo sign), and diffuse loss of the colonic haustrations. There is associated mild engorgement of the pericolic vasa recta and multiple small mesenteric lymph nodes. Small amount of free fluid in the pelvis, but no evidence of free gas. A few loops of small bowel show air-fluid levels, but they are not dilated and have otherwise unremarkable appearances. The liver, spleen, pancreas, kidneys and adrenal glands are normal. No suspicious bone lesions are seen. The lung bases are clear.
Case Discussion
Histology: Sections show colonic mucosa including underlying muscularis mucosae. The biopsy is markedly abnormal, with surface ulceration, reduction in crypt density, areas of crypt destruction, and distortion of architecture. The lamina propria is densely expanded by chronic inflammatory cells, and this is accompanied by a diffuse neutrophilic infiltrate with cryptitis and the occasional crypt abscess. Granulomas are not readily apparent. The deep crypt epithelium shows prominent reactive nuclear hyperchromasia, but definitive cytomegalovirus viral effect is not seen. There is no evidence of dysplasia or malignancy. Immunohistochemistry for CMV is negative.
DIAGNOSIS: Sigmoid biopsy: Moderately severe active chronic colitis. Negative immunohistochemistry for CMV.
Imaging features are suggestive of ulcerative colitis, the main differential is made with Crohn's disease.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.