
This is a basic article for medical students and other non-radiologists
Bowel perforation is an acute surgical emergency where there is a release of gastric or intestinal contents into the peritoneal space.
On this page:
Reference article
This is a summary article; read more in our article on bowel perforation.
Summary
-
epidemiology
- depends on the cause
-
presentation
- history
- may depend on the location of the perforation
- severe and generalised abdominal pain (upper)
- gradual and localised pain (lower)
- anorexia, nausea and vomiting
- may depend on the location of the perforation
- examination
- rigid abdomen and generalised tenderness
- guarding and rebound
- bowel sounds range from quiet to absent
- history
-
pathophysiology
- gastric and duodenal ulceration
- infection (diverticulitis, appendicitis), ischaemia and cancer
- blunt and penetrating trauma
- ingestion of corrosive materials
- iatrogenic causes (ERCP, colonoscopy, laparotomy, biopsy)
-
investigation
- an erect plain radiograph is sensitive for small volumes of free gas
- a supine abdominal radiograph may show signs of free gas
- CT with IV contrast is the gold standard investigation
- free gas and fluid within the peritoneal cavity
-
treatment
- fluid resuscitation and IV antibiotics
- surgical intervention is often required to close the perforation
- bowel resection may be required
- mortality increases the longer surgical treatment is delayed
Role of imaging
- confirm free intraperitoneal gas
- determine the underlying cause
- if possible, identify the site of perforation
Radiographic features
Plain radiograph
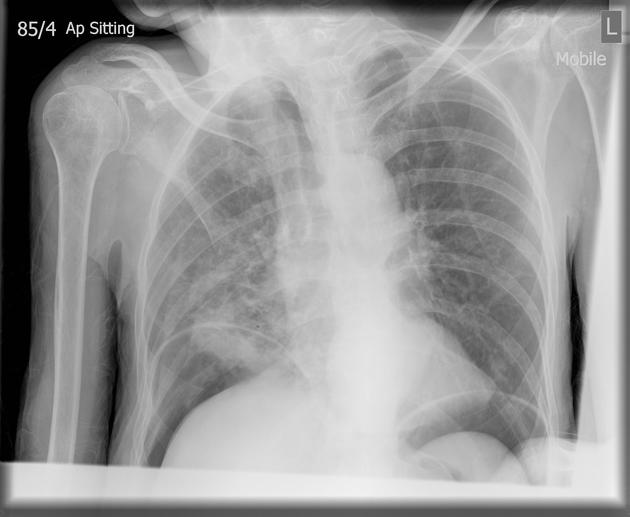
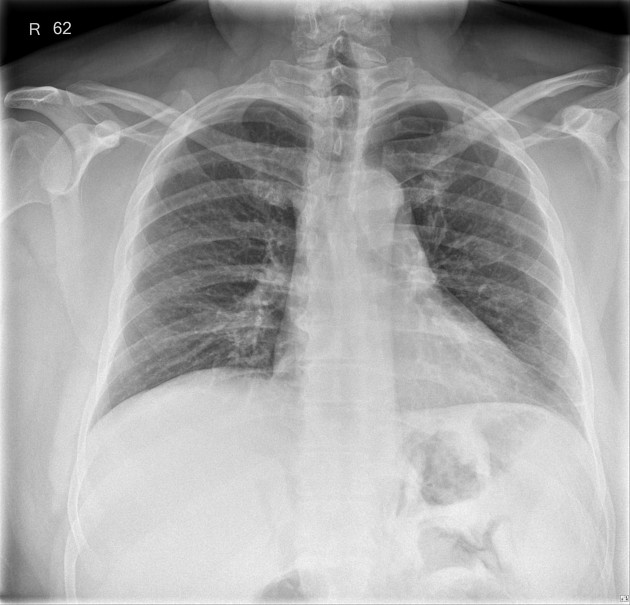
Erect CXR
- very sensitive to even small amounts of gas within the peritoneal cavity
- seen as a crescent under the diaphragm
- summary article: erect chest radiograph
Abdominal X-ray
- performed for other reasons, e.g. to identify bowel obstruction
- several signs of pneumoperitoneum, e.g. Rigler sign
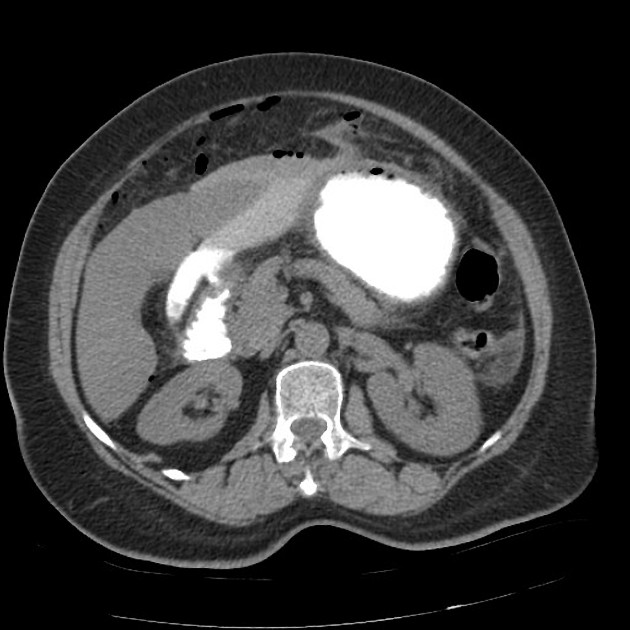
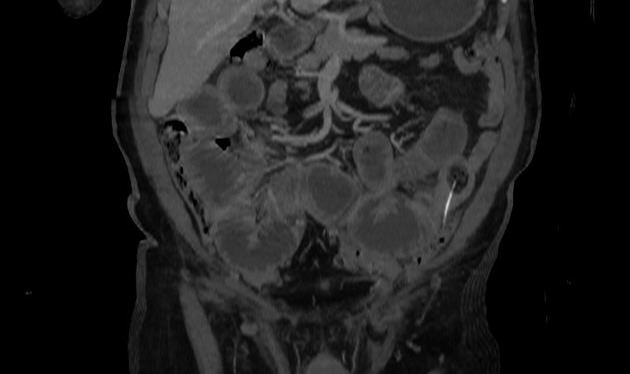
CT
- abdominal CT with IV contrast
- CT is very sensitive for tiny volumes of free gas within the abdomen
- triangles or bubbles or gas out with the bowel
- anti dependant - rising to the top of a cavity, e.g. behind the abdominal wall
- associated fluid within the peritoneal cavity is helpful but non-specific
Finding the cause
CT is also useful to determine the cause of the perforation and is therefore very helpful before surgical intervention.
Where there is more gas than fluid, think lower GI perforation (e.g. sigmoid diverticulitis). Where there is more fluid than gas, upper GI perforation is more likely (e.g. duodenal ulcer).




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.