
Cauda equina syndrome (CES) is considered an incomplete cord syndrome, even though it occurs below the conus. Cauda equina syndrome refers to a collection of symptoms and signs that result from severe compression of the descending lumbar and sacral nerve roots. It is most commonly caused by an acutely extruded lumbar disc and is considered a diagnostic and surgical emergency.
On this page:
Epidemiology
Cauda equina syndrome is rare with prevalence estimated at approximately 1 in 65,000 (range 33,000 to 100,000) 1. It has been estimated to occur in ~1% (range 0.1-2%) of herniated lumbar discs 2,3.
Risk factors
congenital or acquired spinal canal stenosis 3
recent lumbar spinal surgery 2
Clinical presentation
Cauda equina syndrome can present either acutely or chronically and requires two sets of symptoms/signs 1-3:
perianal and "saddle" paresthesia
bowel, bladder and/or sexual dysfunction
There is a host of associated symptoms and signs, which may be unilateral or bilateral and have a variable presence 1-3,6,10:
radiculopathy/sciatica (unilateral or bilateral)
paresthesia of lower limbs and perianal/saddle region (variable)
weakness of lower limbs in a lower motor neuron pattern (variable)
reduction/absence of lower limb reflexes
Additionally, cauda equina syndrome can be classified as incomplete or complete based on the presence of bowel and bladder symptoms 1,2,10:
-
incomplete
may have loss of urgency or decreased urinary sensation without incontinence or retention
accounts for ~40% (range 30-50%) of presentations 6
-
complete
urinary and/or bowel retention or incontinence
accounts for ~60% (range 50-70%) 6
Pathology
Etiology
There is a long list of conditions that can cause cauda equina syndrome (some of these are very rare) 1-3:
-
degenerative
lumbar disc herniation (most common, especially at L4/5 and L5/S1)
lumbar spinal canal stenosis
hemorrhage into a Tarlov cyst 11
-
inflammatory
both acute and chronic form may be seen in long-standing ankylosing spondylitis (2nd-5th decades; average 35 years) 7-9
-
traumatic
spinal fracture or dislocation
epidural hematoma (may also be spontaneous, post-operative, post-procedural or post-manipulation)
-
infective
tuberculosis (Pott disease)
-
tumors
-
primary
-
tumors in vertebral bodies
-
-
vascular
numerous other rare space-occupying lesions (e.g. sarcoid)
Radiographic features
Plain radiograph
limited value; may demonstrate gross degenerative or traumatic bony disease 2
CT
While not the current gold standard for assessment of suspected cauda equina syndrome, research has suggested that CT can reliably exclude cauda equina when thecal sac effacement is <50% 13, and that an optimized CT protocol can accurately identify cases requiring urgent decompression 12. This may be of particular value in healthcare settings with limited access to MRI.
CT myelogram
useful in patients in whom MRI is contraindicated or not available
-
partial or complete blockage of contrast
may demonstrate an "hourglass" shape to the contrast-filled thecal sac incomplete blockage 2
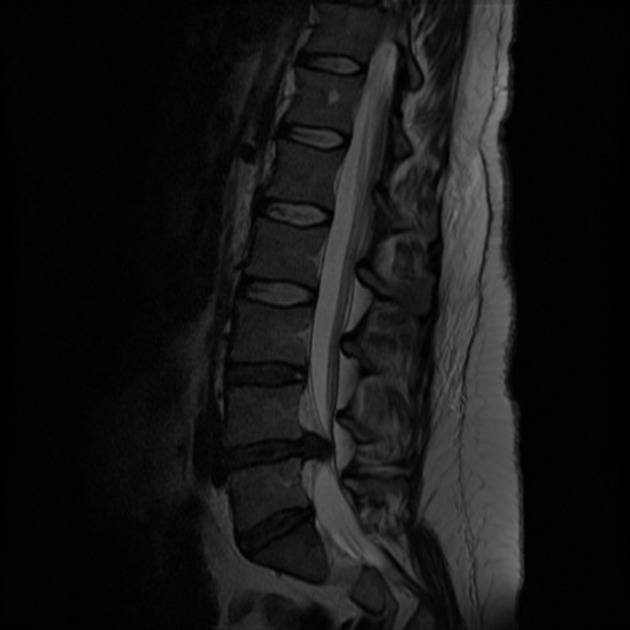
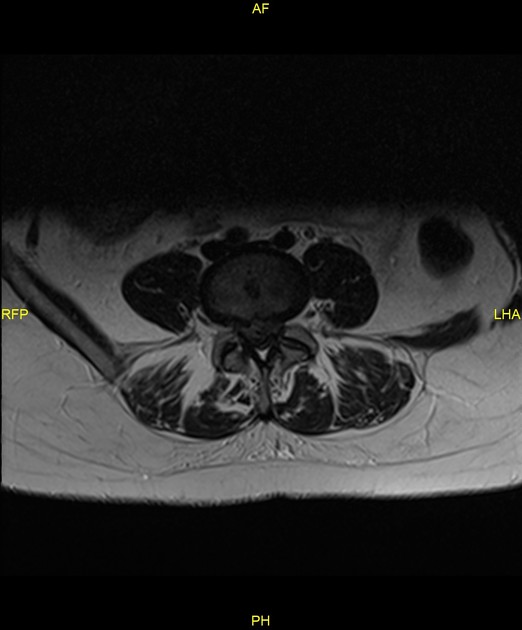
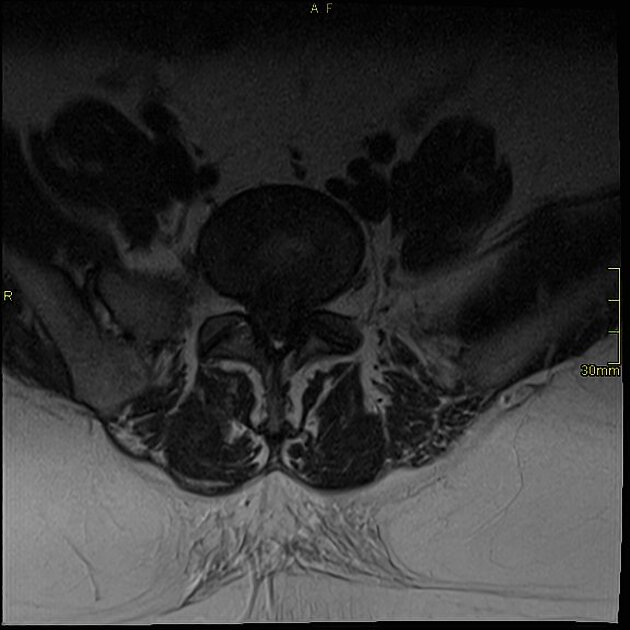
MRI
imaging modality of choice 2,3
sagittal and axial T1 and T2 sequences are usually sufficient 4
post-contrast and STIR sequences may be required if infective causes are suspected 3,4
Treatment and prognosis
Cauda equina syndrome is considered a diagnostic and surgical emergency, although there is some debate about the timing of surgery, which is also dependent on whether the pathology is acute or chronic. Surgical decompression within 24 hours seems to have the best outcome 1,3,6.
Patients with complete cauda equina syndrome have a poorer outcome 3. Approximately 20% of patients will have a poor outcome in terms of urological and/or sexual function, as well as lower limb paresthesia and weakness 6.
Differential diagnosis
Clinically the main differential is that of conus medullaris syndrome.
Practical points
Cauda equina syndrome is a clinical diagnosis; the term should not be used in a radiology report unless the appropriate symptoms and signs are known. In the absence of corroborating history, a better phrasing is "compression of the cauda equina" which should then be correlated clinically. This is an important distinction as many elderly patients may have marked canal stenosis with compression of the cauda equina but do not present acutely with cauda equina syndrome.














 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}