
Croup, also known as acute laryngotracheobronchitis, is due to viral infection of the upper airway by parainfluenza virus or respiratory syncytial virus (RSV).
Although imaging findings are not required for the diagnosis, classic findings of narrowing of the subglottic airway and dilatation of the hypopharynx are supportive of the diagnosis.
On this page:
Epidemiology
Croup can happen in children as young as 6 months up to 15 years old, but most commonly between 6 months to 3 years with a peak at 18 months. It is the most common cause of upper respiratory distress in infants and young children which usually occurs in late fall to early winter 3.
Clinical presentation
Clinically it presents with protracted barking cough and inspiratory stridor due to mucosal edema resulting in tracheal narrowing.
Radiographic features
Plain radiograph
Plain radiographs are not always required, as the diagnosis is often made clinically. They are usually obtained to exclude other causes of a similar presentation. Typical radiographic findings include:
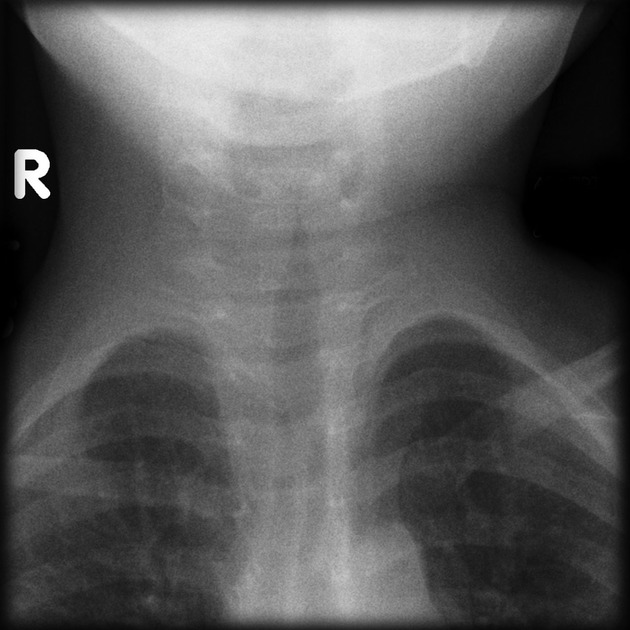
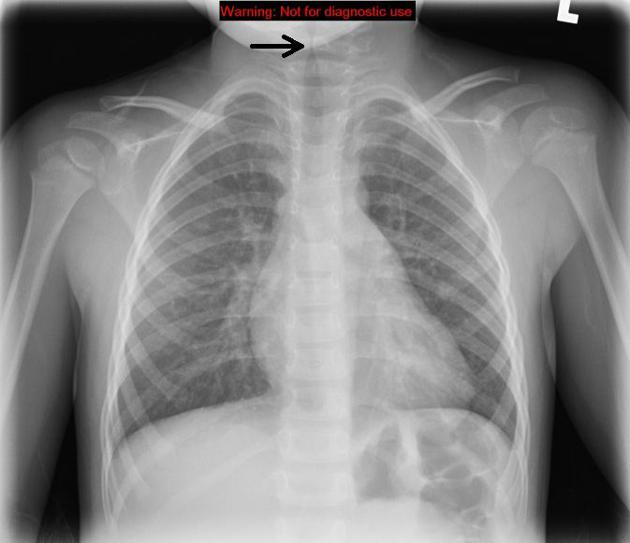
steeple sign (also known as "wine bottle sign" and "inverted V sign"): seen on AP radiographs of the neck or chest and neck demonstrates uniform narrowing of the subglottic airway
-
distension of the hypopharynx is also seen due to the patient's attempt at decreasing airway resistance.
while this can be a sign of upper airway obstruction, note that it also normally occurs at end inspiratory phase in a crying child 5
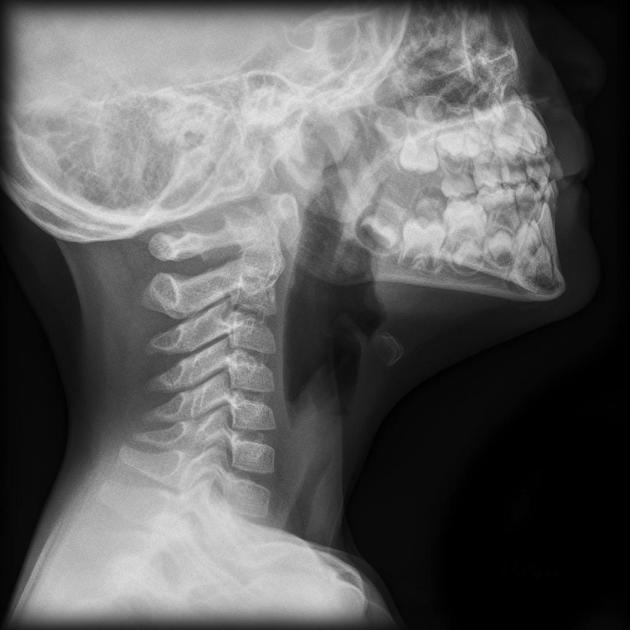
lateral radiograph of the upper airway will show a normal epiglottis and narrowing of the subglottic region
Treatment and prognosis
Croup is usually self-limiting and has a good overall long-term prognosis.
Treatment is directed toward improving air exchange. Supportive measures including corticosteroids and nebulised epinephrine are commonly used.
Differential diagnosis
General imaging differential considerations include:
-
-
enlargement of the epiglottis and aryepiglottic folds (thumb sign)
omega epiglottis (normal variant) can mimic
usually older children
-
congenital subglottic stenosis: different clinical presentation






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.