
The diaphragm is the dome-shaped skeletal muscle that separates the thoracic cavity from the abdominal cavity, enclosing the inferior thoracic aperture.
On this page:
Terminology
On chest imaging, in particular chest radiography, an imaginary anteroposterior midline divides the diaphragm into two halves, forming the left and right hemidiaphragms. The hemidiaphragms are purely descriptive terms and are not discrete anatomical structures.
Gross anatomy
The muscular fibres of the diaphragm originate around the circumference of the inferior thorax and converge to a common insertion point of the central tendon.
The muscle slips can be grouped according to their origins:
sternal: arise from two strips under the xiphoid process
costal: arise from the inner surfaces of the lower six costal cartilages and adjoining ribs, interdigitating with the transversus abdominis muscle
lumbar: arise from the aponeurotic arches (lumbocostal arches) and from the lumbar vertebrae (forming the crura)
All these muscles insert into the central tendon, a thin but strong aponeurosis. It is situated immediately below and is fused to the pericardium. It is within this central tendon that the vena caval hiatus is located, with the tendon allowing the inferior vena cava (IVC) to remain patent during respiration.
Lumbocostal arches
There are two paired posterior tendinous lumbocostal arches:
medial lumbocostal arch (medial arcuate ligament): a tendinous arch from the superior anterior thickened psoas major fascia; continuous medially with the ipsilateral crus; attached to the L1/L2 anterolateral vertebral body, and the anterior aspect of the L1 transverse process
lateral lumbocostal arch (lateral arcuate ligament): covers quadratus lumborum muscle; attaches medially to the L1 transverse process and attaches laterally to the tip of the 12th rib; this may be discontinuous on CT in up to 11% of people and hence may mimic diaphragmatic rupture 8
Crura
The crura are paired tendinous structures of the posterior diaphragm that blend with the anterior longitudinal ligament of the vertebral column:
right crus is longer and broader than the left, and arises from the anterior surfaces of the bodies of L1-3
left crus arises from the corresponding portions of L1-2
The medial margins of the two crura pass forwards and medially. They meet in the midline to form an arch in front of the aorta called the median arcuate ligament.
Apertures
Through the diaphragm are a series of three major and some minor apertures that permit the passage of structures between the thoracic and abdominal cavities:
-
aortic hiatus (T12 level):
-
oesophageal hiatus (T10 level):
formed mainly by the large right crus and its muscular fibres, phrenoesophageal ligament controls the hiatus
oesophagus, vagus nerves, small oesophageal branches of the left gastric vessels, lymphatics
-
vena caval hiatus (T8 level):
junction of the right and middle leaflets of the central tendon
inferior vena cava, right phrenic nerve
-
two in the right crus - transmits the greater and lesser splanchnic nerves
three in the left crus - transmits the greater and lesser splanchnic nerves, and also hemiazygos vein
under the medial arcuate ligament: sympathetic trunks
under the lateral arcuate ligament: subcostal nerves and vessels
left phrenic nerve pierces the dome of the left hemidiaphragm
-
small defect between the sternal and costal slips of muscles
superior epigastric vessels course through this area
The vertebral levels of the three main diaphragmatic apertures can be remembered by this mnemonic.
Arterial supply
costal margins: lower five intercostal arteries; subcostal arteries
abdominal surface: right and left inferior phrenic arteries (from abdominal aorta) 4
supply is augmented by the superior phrenic, musculophrenic and pericardiophrenic arteries 5
Venous drainage
right inferior phrenic vein into the inferior vena cava (IVC)
left inferior phrenic vein into the left suprarenal vein or left renal vein
Innervation
Innervation is mainly via the bilateral phrenic nerves (C3-C5) which pierces the diaphragm and on its inferior surface divide into several radiating branches to supply it.
each phrenic nerve (C3-C5) provides the sole motor supply to the ipsilateral hemidiaphragm 9,10
sensory innervation to the central tendon region is supplied by the phrenic nerves 9,10
sensation innervation to the peripheral diaphragmatic pleura is supplied by the lower 5-6 intercostal nerves whereas the central pleura is from the phrenic nerves
the lower 5-6 intercostal nerves supply proprioceptive fibres to the margins of the diaphragm 4
Movement
The major role of diaphragmatic contraction is during inspiration to increase the volume of the thoracic cavity, but it is also used in abdominal straining.
Variant anatomy
scalloped or serrated appearance: due to individual muscle slips 7
dromedary diaphragm (hump)
accessory diaphragm
connection with transversus abdominis muscle
sternal portion of the diaphragm may be absent
extension of muscle fibres onto the quadratus lumborum muscle
hemiazygos vein may run through the aortic hiatus
azygos vein may run through the right crus
Radiographic features
Plain radiograph
The right dome of diaphragm is usually 2cm higher than the left dome 11.
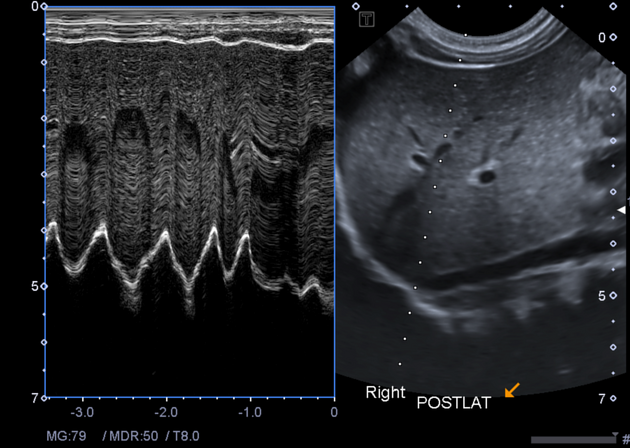
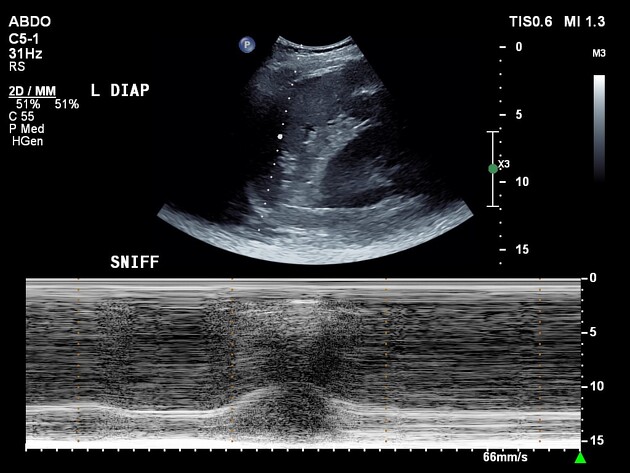
Ultrasound
Diaphragm is seen as echogenic line covering the upper surface of liver and spleen 11.
Development
The diaphragm embryologically develops from four main sources:
-
produces most of the central tendon and contributes to the ventral mesentery in the gut
-
cervical myotomes (3rd to 5th):
infiltrates the septum transversum with muscle cells
carries their own nerve supply from these levels explaining the C3-C5 origin of the phrenic nerve
-
mesodermal folds which connect the septum transversum to the pericardioperitoneal canals
separates the peritoneal and pleuropericardial cavities
dorsal oesophageal mesentery



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}