Finger pulley injuries can occur at any one of the five flexor tendon pulleys of the fingers, but most commonly affects the A2 pulley.
On this page:
Clinical presentation
These are overwhelmingly the result of a discrete trauma occurring with the hand in a finger grip position. They are most frequently seen in competitive climbing athletes, up to a quarter of whom report finger pulley injuries.
Pathology
The annular pulleys are the most functionally important and commonly injured. They comprise a transversely oriented sheath of fibrous tissue that wraps over the flexor digitorum superficialis and profundus tendons.
There are five flexor tendon pulleys in the fingers that are named A1-A5. The thumb only has two pulleys that are described as A1 and A2.
-
A1, A3, and A5 pulleys
overlie the palmar aspect of the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints respectively
attach to the volar plate
rarely torn
-
A2 and A4
attach to periosteum
A2 is most load-bearing and most frequently torn 2
A4 is the most flexible
A4 rupture often seen with A3 rupture
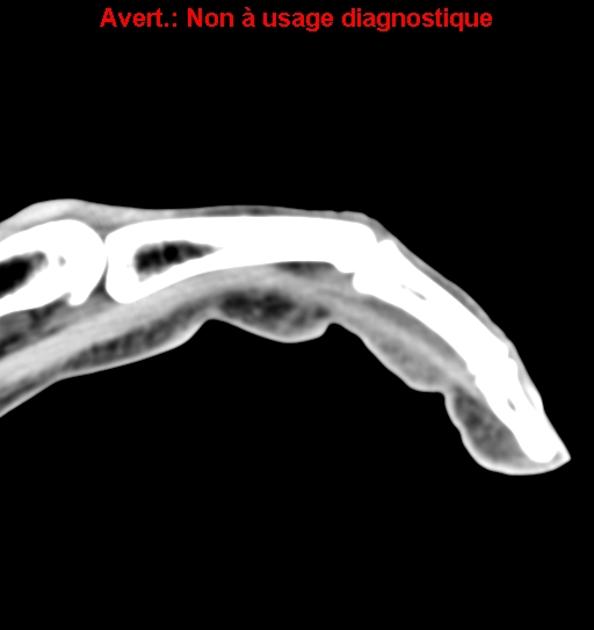
Radiographic features
Plain radiograph
Plain radiographs have no role in the diagnosis but may be requested in the acute setting of a finger injury. May show soft tissue swelling.
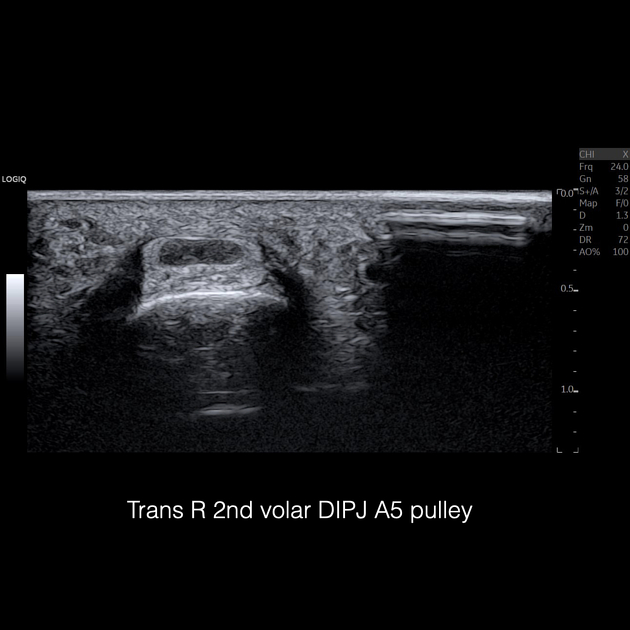
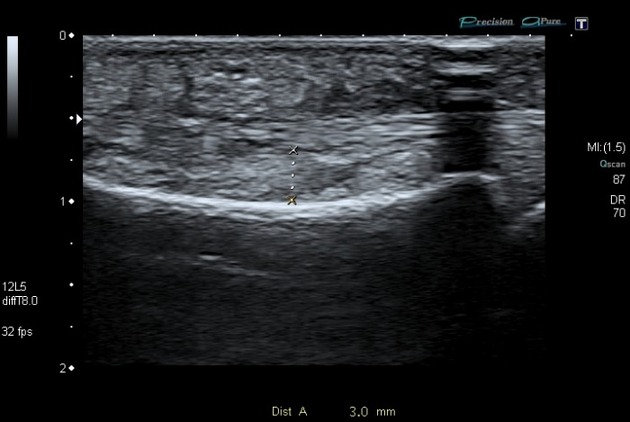
Ultrasound
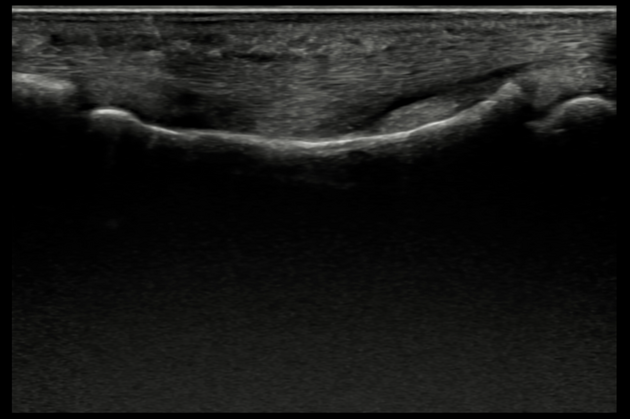
Ultrasound allows for dynamic testing with flexion stress on the affected digit. It is reported to be up to 100% accurate in identifying pulley injuries 3,4. Normal pulleys are seen as thin fibrillar, hyperechoic bands anteriorly while their lateral portion is usually obscured by anisotropy.
-
pulley rupture
hematoma or discontinuity in the pulley band
bowstringing of the flexor digitorum tendon
displacement of the flexor digitorum profundus from the phalangeal/metacarpal cortex
-
pulley sprain or partial rupture
pulley thickening
hypoechoic change
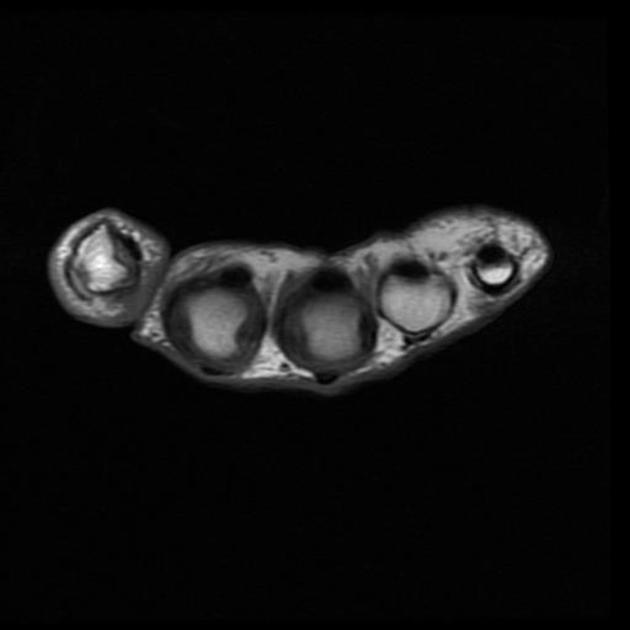
MRI
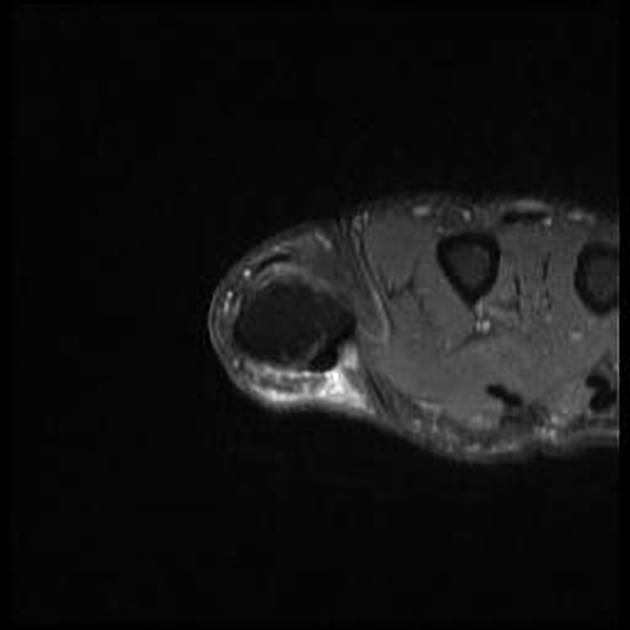
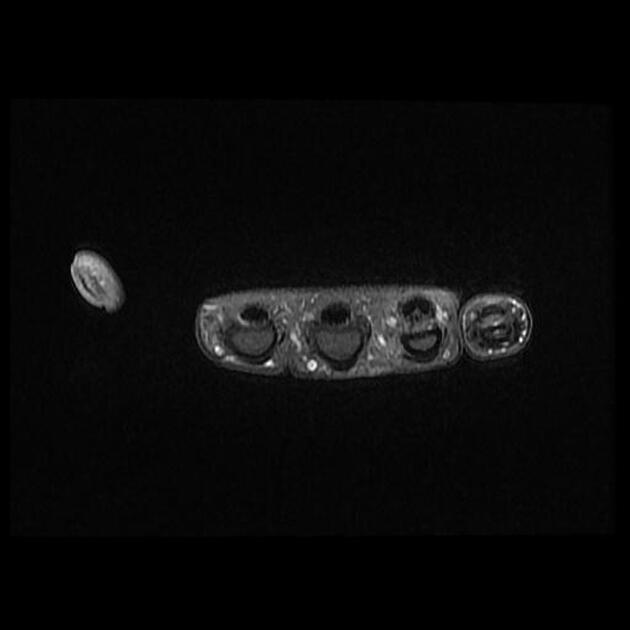
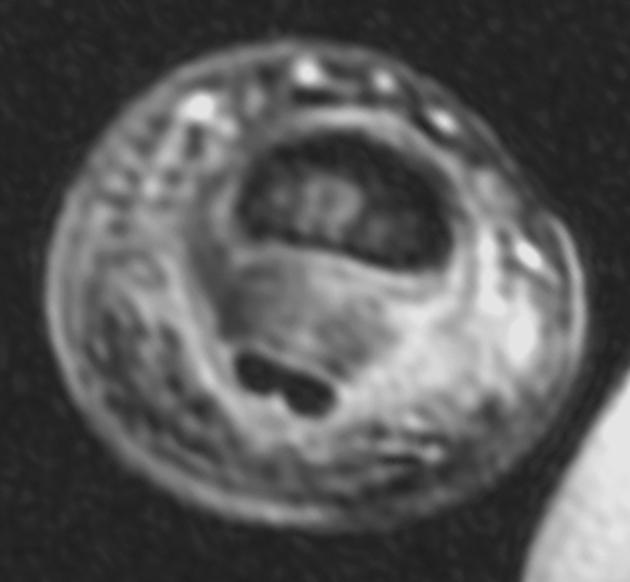
MRI is also highly accurate for finger pulley injuries. MRI is better at demonstrating the lateral pulley attachments, best seen on axial slices. The hand can be scanned in a normal and stressed position.
The pulleys are normally seen as bands of hypointense tissue and are best appreciated on T1 imaging without fat saturation. Fluid sensitive imaging helps demonstrate associated focal edema at the site of injury.
Treatment and prognosis
Injury to a single pulley can be managed conservatively. When multiple pulleys are ruptured surgical repair is often required 7.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.