
Infective endocarditis is defined as infection of the endocardium. It commonly affects the valve leaflets and chordae tendineae, as well as prosthetic valves and implanted devices.
On this page:
Epidemiology
Infective endocarditis has an estimated general prevalence of 3 to 9 cases per 100,000. Intravenous drug users are at increased risk with approximately 2 cases per 1000 in this patient group. It is more common in men than women (>2:1). In the general population, it affects more individuals older than 65 years 1.
Diagnosis
See the separate article on the Duke criteria for infective endocarditis.
Clinical presentation
ECG
Non-specific, but electrocardiographic abnormalities common and may include:
-
prolongation of the PR interval
with progressive degrees of AV block
sinus tachycardia
bundle branch blocks
-
left or right ventricular strain pattern
voltage criteria for hypertrophy with regional ST depression and T wave inversion
may be secondary to conduction system invasion or underlying predisposition (e.g. aortic stenosis)
Pathology
The following conditions appear to play critical roles in the creation of an endocarditic lesion 1:
-
endocardial abnormality
endocardial inflammation
endothelial injury from central lines and other forms of cardiovascular instrumentation
valvular disease including prosthetic valves
-
bacteremia
microorganism access to the bloodstream from oral, genitourinary, or gastrointestinal sources
trauma
intravenous and subcutaneous injections
-
microbial properties and associated components
microbial virulence properties such as adhesion proteins and tissue-destructive factors
microbial quantity
particulate and diluent materials
repetition of microbial entry into the bloodstream
Once the endocarditic lesion is initiated, the clotting pathway catalyzes vegetation formation. The microbes become buried in the vegetation and may form a biofilm around them, thereby becoming inaccessible to immune cells or antibiotic drugs for clearance and eradication. Endocarditic vegetation is the pathologic hallmark of infective endocarditis and commonly appears as an irregular, mobile or fixed mass and is usually attached to the endocardium on the low-pressure side of a valve, chordae tendineae or ascending aorta. Vegetation fragments can break off and undergo embolization, causing more conspicuous clinical signs and symptoms of infection like pneumonia and stroke.
Radiographic features
Plain radiograph
Chest radiographic findings are non-specific and may show opacities suggestive of underlying pneumonia and septic pulmonary emboli. Patients with valve leaflet destruction may manifest with signs of congestive heart failure. The cardiac silhouette may be enlarged due to pericardial effusion. Some patients may also show pleural effusion.
Ultrasound
Echocardiography
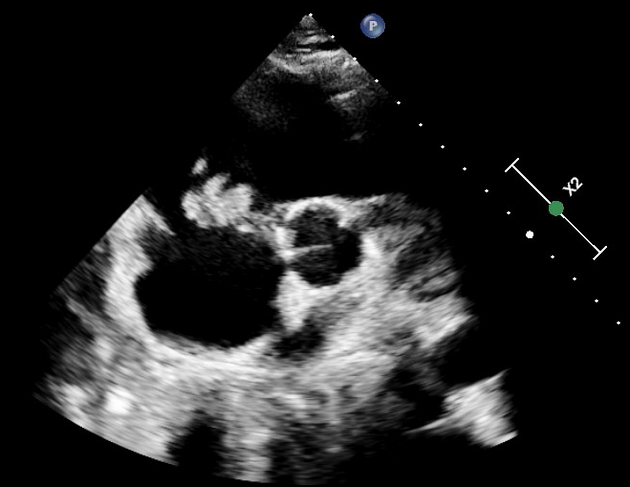
Echocardiography is the primary imaging modality of cardiac infections. It has been integrated into the Duke criteria for diagnosis of infective endocarditis. Transesophageal echocardiography is superior to transthoracic investigations; the latter should only be used as a screening modality in low-risk patients with a low pre-test probability/clinical suspicion 9.
Vegetations have the following cardinal features on echocardiography 8:
isoechoic to tissue
independent movement
-
preferentially congregate on the leading edge of the valve
-
on the lower-pressure side of the valve
most common location of mitral valve involvement would be the anterior leaflet of the mitral valve on the atrial side of the MV
in prosthetic valves, however, they will most commonly be located at the junction between the sewing ring and the valvular annulus
-
-
associated with valvular regurgitation
-
vast majority cause failure of leaflet coaptation
-
may also perforate valve, which will appear as an endocardial discontinuity
often results in multiple, aliased regurgitant jets on the high-pressure side of the affected valve
-
argues against infective endocarditis if regurgitation jet is not present
-
Other possible echocardiographic findings:
-
valvular stenosis
vegetations may, less commonly, obstruct valves
dehiscence of prosthetic valve
-
jet vegetations
secondary locus of vegetations where regurgitant jet meets the endocardium
-
pseudoaneurysm
anechoic space with pulsatile flow
communicates with the cardiac chamber lumen
-
abscess
irregular collection of heterogeneous echogenicity directly adjacent to the affected valve
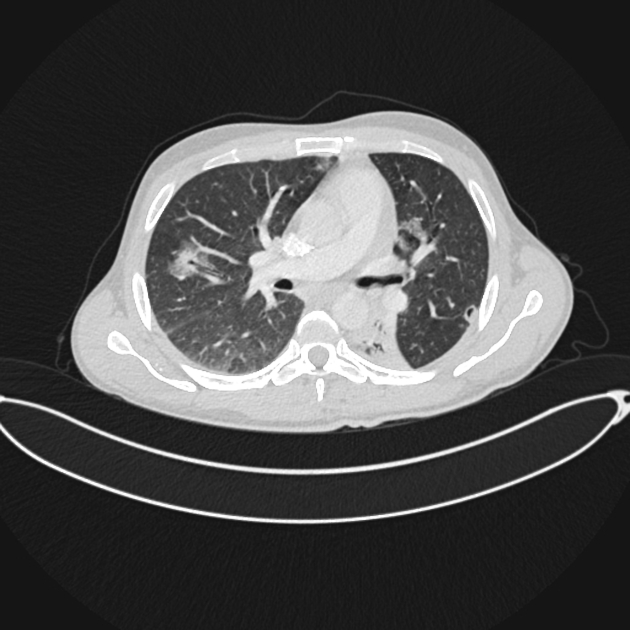
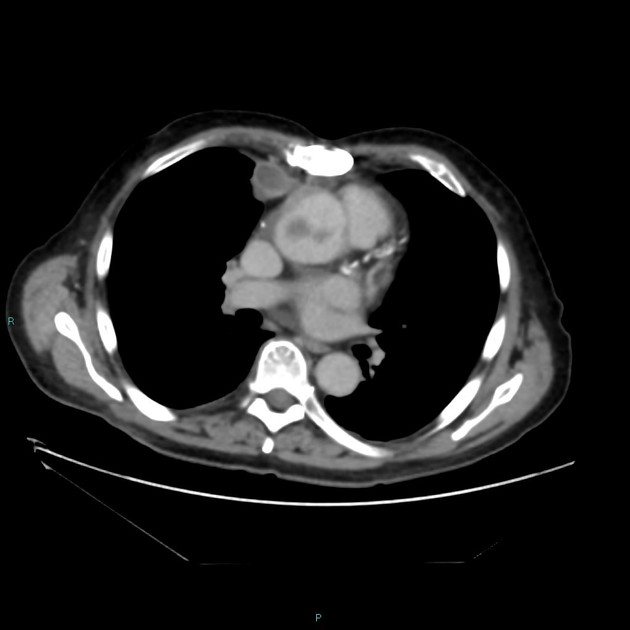
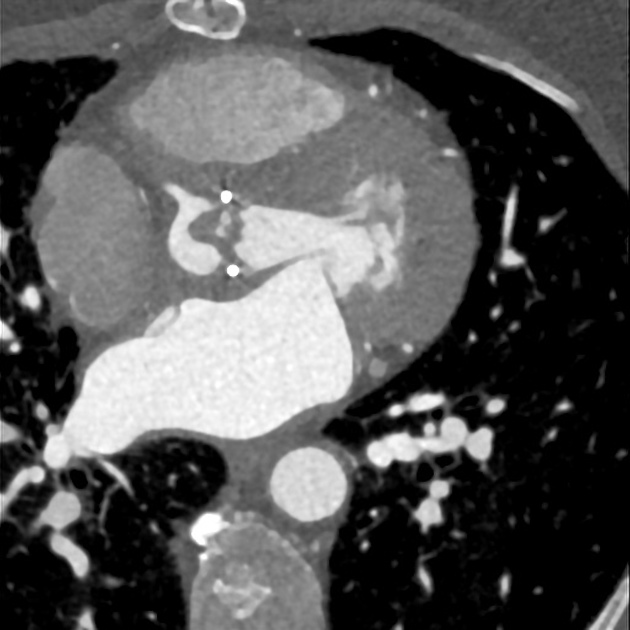
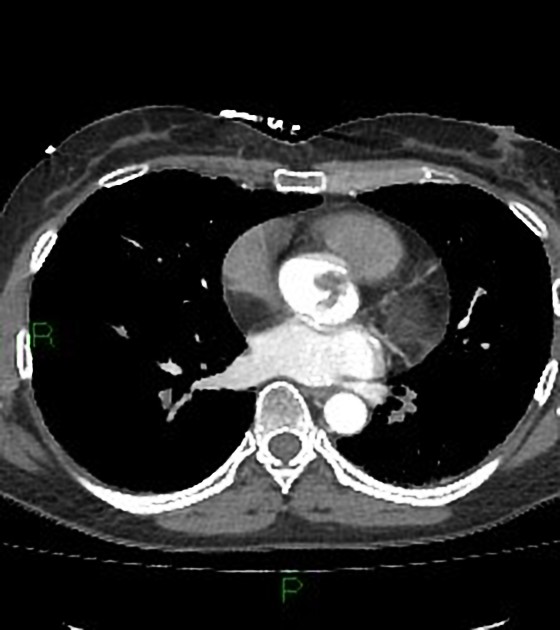
CT
Cardiac CT angiography may demonstrate endocarditic vegetations as hypoattenuating filling defects surrounded by intravenous contrast material. Cardiac-gated CT angiography can also demonstrate valve tissue destruction and perivalvular extension with pseudoaneurysm or fistula formation. CT may miss small vegetations.
MRI
Cardiac MRI can detect valvular vegetation features of infective endocarditis. The appearance of vegetations depends on the imaging sequence used and ranges from low to intermediate signal intensity and isointense to muscle with balanced steady-state free precession (SSFP) and inversion-recovery sequences. Post-gadolinium images may show enhancement of the vegetations and abscess. In the absence of vegetations, MRI can demonstrate delayed enhancement representing endothelial inflammation of the cardiovascular structures, which can contribute to the diagnosis and treatment planning of infective endocarditis 2. Cardiac MR imaging also allows quantification of regurgitation fraction.
Treatment and prognosis
Infective endocarditis is a disease with high morbidity and mortality, even with appropriate diagnosis and therapy 3. With treatment, which includes antibiotics and surgery, the mean in-hospital mortality of infective endocarditis is 15-20% with 1-year mortality approaching 40% 1. If untreated, infective endocarditis is invariably fatal.
Complications
Septic emboli occur in 12-40% of infective endocarditis cases 3. They can affect any organ or tissue in the body with an arterial supply:
central nervous system (most common)
lungs (especially in right-sided infective endocarditis)
spleen
kidneys
liver
musculoskeletal system
Other complications:
paravalvular, annular or aortic abscess / aortic root abscess
mycotic aneurysms, including intracranial mycotic aneurysms
heart block
valve dehiscence or severe dysfunction
Differential diagnosis
Differential diagnosis of vegetations include:



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}