
Morquio syndrome (in older literature it is sometimes called Morquio-Brailsford syndrome) is an autosomal recessive mucopolysaccharidosis (MPS) type IV.
On this page:
Epidemiology
Incidence is estimated at ~1:40,000.
Clinical presentation
Many cases present at ~2 years of age and have normal intelligence. Clinical features:
severe dwarfism (<4 foot)
joint laxity
corneal opacification/clouding
lymphadenopathy
progressive deafness
spinal kyphoscoliosis
prominent mandible and lower face
short neck
Pathology
It results from an excess of keratan sulphate due to a deficit in its degradation pathway. Keratan sulphate accumulates in various tissues inclusive of cartilage, the nucleus pulposus of the intervertebral discs and corneas.
Radiographic features
Plain radiograph / CT
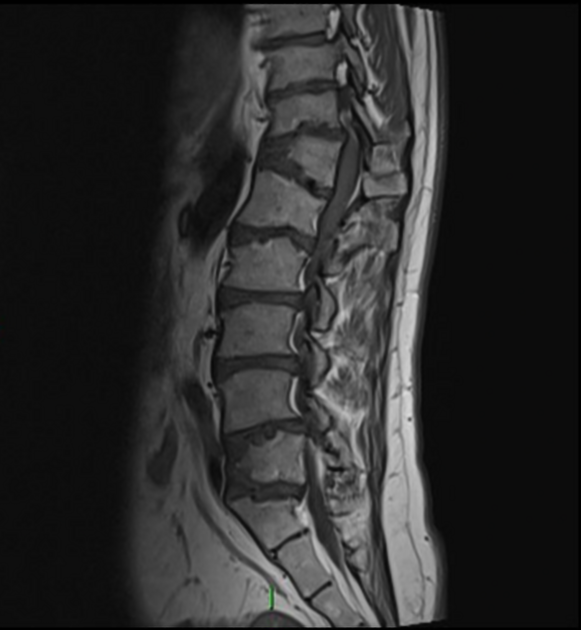
Axial manifestations
hypoplasia of odontoid peg
round vertebral bodies
goblet shaped flared iliac wings, increased acetabular angles and constricted iliac bone base
Calvarial manifestations
Peripheral musculoskeletal manifestations
short and wide tubular bones
metaphyseal flaring in long bones
multiple epiphyseal centers
wide metacarpals with proximal pointing of index to little finger
irregular carpal bones
flattened proximal femoral epiphyses; risk of lateral subluxation and dislocation
Thoracic manifestations
anterior sternal bowing, increased AP chest diameter, wide ribs
Ultrasound
Echocardiography
late-onset aortic regurgitation
Treatment and prognosis
Life expectancy ranges between 30-40 years. The most common cause of death is cervical myelopathy from C2 abnormality. Patients are also particularly vulnerable to respiratory infection.
History and etymology
Named after Luis Morquio, an Uruguayan pediatrician (1867-1935) published his first case in 1929 5. James Brailsford (1889-1961) 6 a renowned British radiologist made an important contribution to the understanding of the radiographic appearances of this condition, and also published his first case in 1929, independently of Morquio 8.







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.