
Renovascular hypertension is a type of secondary hypertension, where high blood pressure develops secondary to renal artery disease.
On this page:
Epidemiology
Approximately 2.5% (range 0.5-5%) of hypertensive patients will have renovascular hypertension as a cause 2,3.
Pathology
The core pathophysiology behind renovascular hypertension is a reduction in renal perfusion. Low perfusion creates a cascade in which the juxtaglomerular apparatus detects reduced blood flow, leading to increased renin-angiotensin-aldosterone system (RAAS) activity 6.
Etiology
Several conditions can cause renovascular hypertension with the most common being atherosclerotic renal artery stenosis (~90%) and fibromuscular dysplasia (second most common) 1-3.
Other causes can cause renovascular hypertension but are much rarer 2,3:
renal artery dissection (e.g. from trauma or aortic dissection)
renal artery embolism or thrombosis
EVAR stent graft
encircling tumor (e.g. pheochromocytoma)
radiation-induced fibrosis
Radiographic features
Nuclear medicine
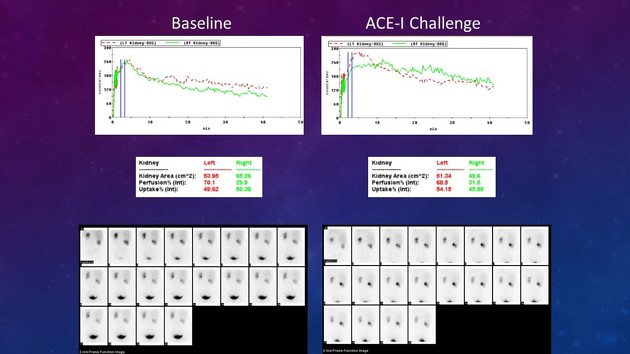
The appearance of renovascular hypertension on nuclear renography will differ depending on the radionuclide used and will trace glomerular filtration rate (GFR) or tubular secretion, or both.
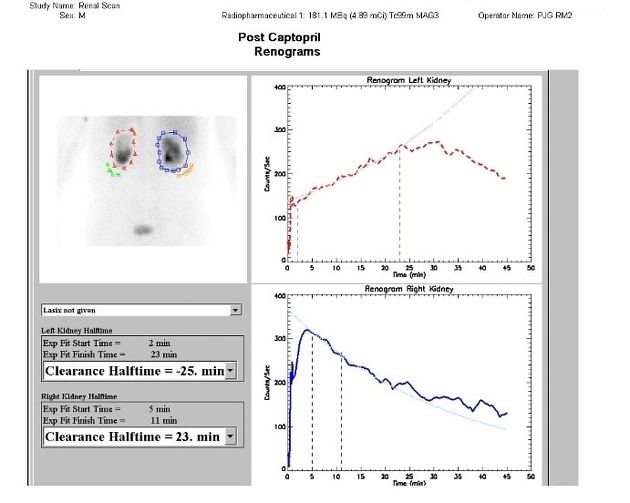
In cases of significant renal artery stenosis, nuclear renography may appear abnormal, however, in less severe cases it may appear normal due to physiologic homeostasis of the renin-angiotensin axis. As such, imaging is typically performed with both a baseline renogram as well as a captopril renogram.
In patients with renovascular hypertension, the ACE inhibitor will prevent modulation of the efferent vasculature and GFR will drop in the affected kidney. For radiotracers with tubular secretion, tracer will build up in the kidney, but the drop in GFR will prevent it from being drained into the bladder and the radiotracer will continue to accumulate 4.
Treatment and prognosis
Treatment of the underlying cause has variable effect 2. Renovascular hypertension can lead to ischemic nephropathy and end-stage renal failure 3.




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.