
A Roux-en-Y gastric bypass is one of the most common bariatric surgeries, used to treat morbid obesity.
In this laparoscopic operation, the stomach is stapled or divided to form a small pouch (typically <30 mL in volume), which is anastomosed to the Roux limb (also known as the efferent or alimentary limb) made of jejunum of varying length (typically 75-150 cm).
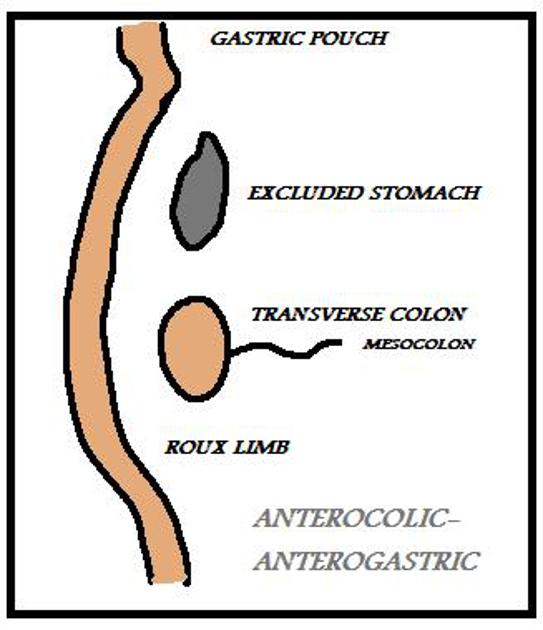
The Roux limb may be brought up to the gastric pouch in two ways:
anterior to the transverse colon (antecolic-anterogastric)
posterior to the transverse colon (retrocolic-retrogastric)
The excluded gastric remnant remains attached to the duodenum and proximal jejunum, which make up the hepatobiliary limb (also known as the afferent limb). The hepatobiliary limb is then anastomosed to the Roux limb forming a jejunojejunal anastomosis. The hepatobiliary limb and Roux limb anastomose in a Y-shaped configuration. Distal to this, the small bowel as it runs to the ileocecal valve is known as the common channel.
Thus, there are two anastomoses: a proximal gastrojejunal anastomosis and a distal jejunojejunal anastomosis.
On this page:
Radiographic features
CT
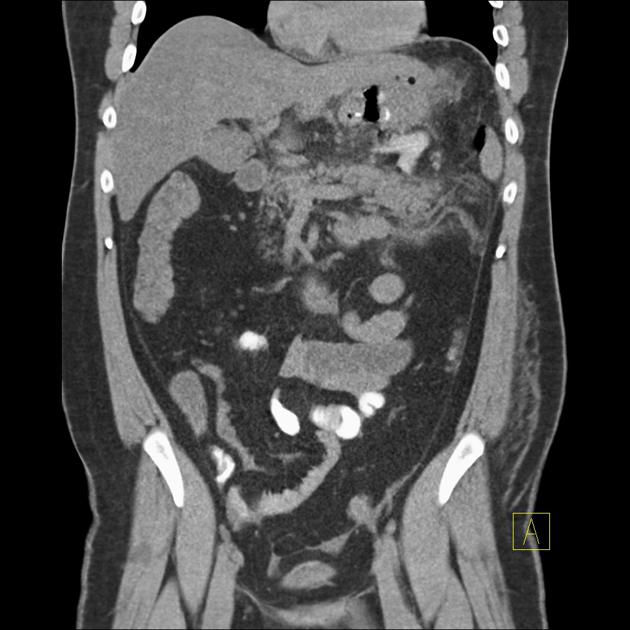
After the bypass surgery, a CT scan should be undertaken with intravenous and oral contrast agents 9. Positive oral contrast is given just before the scan in order to differentiate the gastric pouch and Roux limb from unopacified stomach and biliopancreatic limb 9.
Complications
Early
Early complications of gastric bypass surgery include 3:
anastomotic leak: usually at the gastrojejunal anastomosis
acute ischemia
Late
-
anastomotic narrowing/stenosis/stricture
the most common cause of postoperative nausea and vomiting
may require lateral or steep oblique views to visualize
rare at jejunojejunal anastomosis (0.9%)
-
etiology and management vary depending on the location 9
at gastrojejunal anastomosis: tends to be transitory, due to edema or spasm
at jejunojejunal anastomosis: tends to be a well-established stenosis, due to fibrosis or chronic ischemia (therefore, they may require surgery)
gastrogastric fistula (unintended communication between the gastric pouch and excluded gastric remnant)
hemorrhage/hematoma
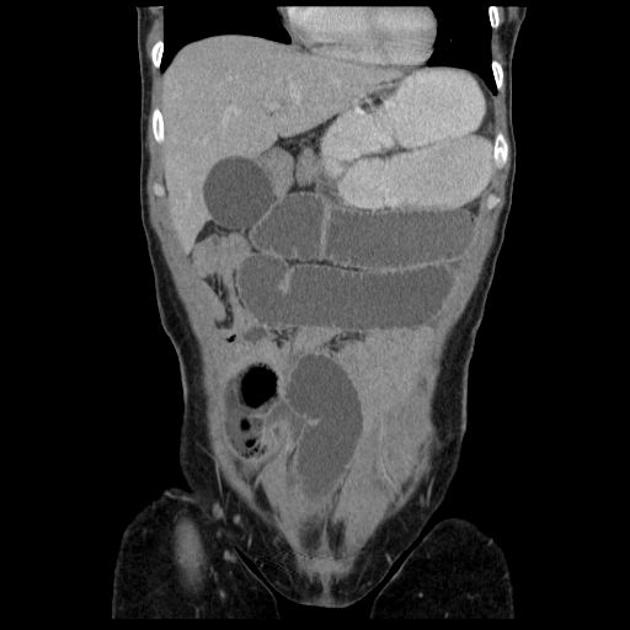
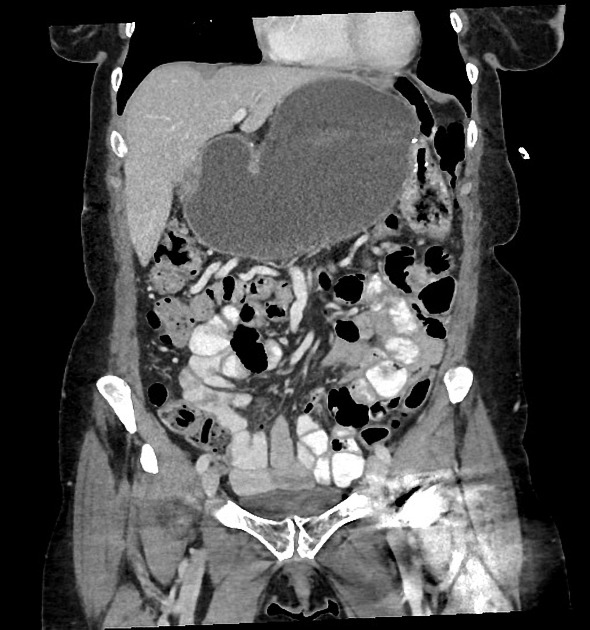
adhesions, potentially leading to small-bowel obstruction
-
higher rate of occurrence with a retrocolic approach
small bowel intussusception, retrograde much more often than antegrade 5-7
bezoar formation in the gastric pouch
History and etymology
The Roux-en-Y is named after the Swiss surgeon César Roux (1857-1934), who was Chief of Surgery at the county hospital of Lausanne and following the opening of the new University of Lausanne, in 1890, was its inaugural Professor of External Pathology and Gynecology 4.










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.