Tibialis posterior dysfunction is common, mostly affecting middle-aged and elderly females, and can progress to adult-acquired flatfoot disease.
On this page:
Pathology
Dysfunction occurs secondary from repetitive overloading resulting in degeneration, which occurs in the typical continuum of tenosynovitis and tendinosis progressing to partial and full-thickness tendon tears. Elongation can also occur without tearing, with as little as 1 cm of elongation resulting in dysfunction 1.
Tibialis posterior can tear in its 1:
- supramalleolar part (uncommon)
- retromalleolar part
- inframalleolar part (most common)
Etiology
Tibialis posterior dysfunction can be secondary to 3:
- trauma
- underlying disease, e.g. inflammatory arthropathy
- idiopathic
- functional, e.g. tarsal coalition
Risk factors
- congenital pes planus
- accessory navicular or cornuate navicular
- obesity
- diabetes
- gout
- inflammatory arthropathy
- hypertension
- corticosteroid use
Radiographic features
Plain radiograph
Secondary features of tibialis posterior dysfunction include 1:
- soft tissue swelling
- navicular tuberosity enthesopathy
- retromalleolar groove bone hypertrophy
- in some cases, there may be subtalar arthritis
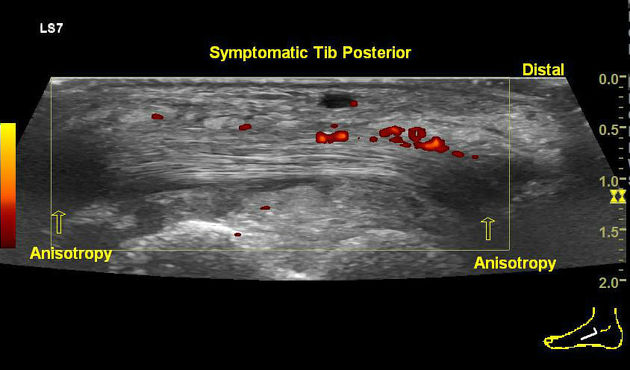
Ultrasound
- tendon sheath effusion and diameter >7 mm reflects tenosynovitis 1
Associations
In advanced posterior tibial tendon injury, increased force is transmitted to other stabilizers of the medial longitudinal arch of the foot. Associations include:
- spring ligament injury
- sinus tarsi syndrome
- plantar fasciitis





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.