
Ulnar impaction syndrome, also known as ulnar abutment or ulnocarpal impaction or loading, is a painful degenerative wrist condition caused by the ulnar head impacting upon the ulnar-sided carpus with the injury to the triangular fibrocartilage complex (TFCC).
Differentiation from ulnar impingement syndrome is critical, which is due to a shortened ulna that abuts and causes radial remodeling.
On this page:
Epidemiology
Ulnar impaction syndrome most commonly presents in middle-aged patients. The majority of cases occur in association with positive ulnar variance or increased dorsal tilt of the distal radius. This can be seen in patients with:
distal radial fracture malunion
ulnar styloid fracture nonunion
radial head resection (such as following an Essex-Lopresti fracture-dislocation)
premature radial physeal closure
congenital wrist abnormalities
Ulnar impaction syndrome is rare in the absence of such anatomic predispositions but can occur if there is excessive repeated loading of the ulnar-carpus in daily activity 5.
Clinical presentation
Patients present with chronic or subacute ulnar-sided wrist pain exacerbated by activity. There is often associated swelling and limitation of forearm and wrist movement. Anything that results in a relative increase in ulnar variance such as firm grip, pronation, and ulnar deviation of the wrist, can exacerbate the symptoms.
Pathology
As the name suggests, ulnar impaction syndrome involves impaction of the distal ulnar upon the ulnar-sided carpal bones, particularly the lunate. This results in a continuum of pathologic changes which are represented in the class II subsection of the Palmer classification of TFCC lesions 2.
IIA TFC complex wear
IIB TFC complex wear, lunate or ulnar chondromalacia
IIC TFC complex perforation, lunate or ulnar chondromalacia
IID TFC complex perforation, lunate or ulnar chondromalacia, lunotriquetral ligament perforation
IIE TFC complex perforation, lunate or ulnar chondromalacia, lunotriquetral ligament perforation, ulnocarpal osteoarthritis
Chronic abutment leads to tears and osteoarthritis of the TFCC.
Radiographic features
Imaging findings of ulnar impaction may precede the onset of symptoms. Recognizing the distribution pattern (ulnar, lunate, triquetral) is the key to making the diagnosis.
Plain radiograph
Plain radiographs can appear normal in early disease. General features include:
-
presence of a predisposing factor
previous distal radial fracture with shortening or dorsal tilt
distal radial resection
-
subchondral sclerosis and cysts in specific ulnar impaction distribution
distal ulna
proximal ulnar aspect of lunate - (see subchondral cyst of the lunate)
radial aspect of triquetrum
ulnocarpal osteoarthritis in more advanced disease
To accurately access ulnar variance, the wrist must be correctly neutrally positioned with the shoulder abducted at 90° and the elbow flexed at 90°. Variance can falsely be reduced in supination and exaggerated in pronation or with clenching of the fist.
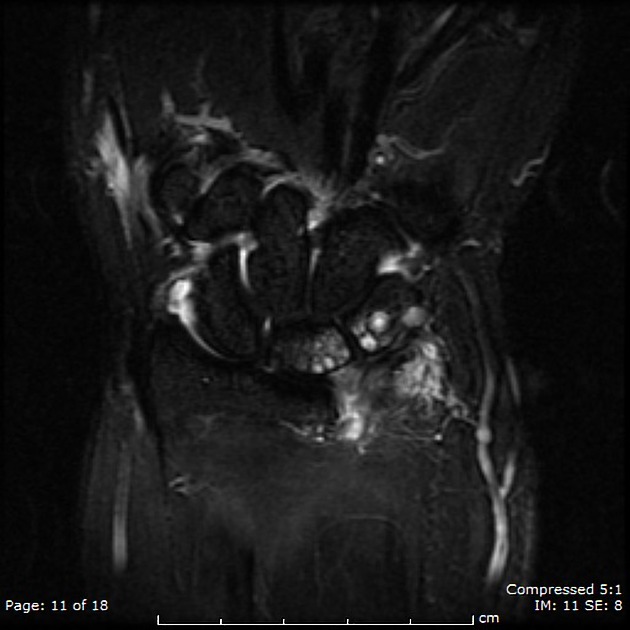
MRI
MR imaging is the investigation of choice in both the detection of early disease and characterization of more advanced disease. Can demonstrate the bone, cartilage and ligamentous features of the syndrome 3.
Location of bone signal changes 4:
ulnar side of proximal lunate ~90%
radial side of proximal triquetrum ~40%
distal ulna ~10%
Types of bone signal change:
subchondral sclerosis (low T1 and T2) most common in lunate
bone edema (high T2, low-intermediate T1)
subchondral cysts (round T2 hyperintensities)
Cartilage and ligamentous changes:
chondromalacia of distal ulnar cartilage (altered signal)
central TFCC signal increase often with tear (T2 hyperintense fluid)
lunatotriquetral ligament tear (T2 hyperintense fluid) with proximal arc offset
Treatment and prognosis
Treatment varies depending on the amount of ulnar variance, the Palmer lesion class, the contour of the distal ulnar and the presence of lunotriquetral instability.
Palmer class IIA and IIB lesions (no TFC perforation) are managed with open wafer procedure (surgical resection of the distal 2-3 mm of the dome of the ulnar head) or formal ulnar shortening (excision of a 2-3 mm slice of the ulnar shaft followed by fixation).
When the TFC is perforated (Palmer class IIC and IID lesions), the head of the ulna can be burred down with the help of arthroscopic instrumentation (arthroscopic wafer procedure). This procedure is minimally invasive, highly effective, and allows rapid return to normal activities.
Class IIE lesions are managed with salvage procedures such as complete or partial ulnar head resection (Darrach procedure) or arthrodesis of the distal radioulnar joint with distal ulnar pseudoarthrosis (Sauve-Kapandji procedure).
Differential diagnosis
-
signal change in lunate is usually more diffuse and radial sided
no ulnar or triquetral abnormality
more often with negative ulnar variance
traumatic TFCC injuries
-
degenerative arthritis of the wrist (SLAC wrist)
radiocarpal joint involved
-
usually radial side of the lunate or distal lunate









 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![[–]](/articles/trapezium-fracture?embed_domain=hackmd.io%25252f%252540yipuafecsl2jsu8smr5njq%25252fbnjhjgjghjghjghradiopaedia-icon-144.pngradiopaedia-icon-144.png&lang=us){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}