
Walled-off pancreatic necrosis (WOPN) is a late complication of acute necrotising pancreatitis, although it can occur in chronic pancreatitis or as a result of pancreatic trauma. Differentiation of WOPN from pancreatic pseudocyst is essential because management differs. WOPN may need aggressive treatment to avoid complications.
WOPN usually occurs four weeks after the episode of acute pancreatitis. Before this time, it is referred to as an acute necrotic collection (ANC).
On this page:
Terminology
The following are the latest terms according to the updated Atlanta classification to describe fluid collections associated with acute pancreatitis 10,11:
-
fluid collections associated with interstitial oedematous pancreatitis (i.e. minimal or no necrosis)
acute peripancreatic fluid collections (APFC): in the first 4 weeks: non-encapsulated peripancreatic fluid collections
pseudocysts: develop after 4 weeks; encapsulated peripancreatic or remote fluid collections
-
fluid collections associated with necrotising pancreatitis
acute necrotic collections (ANCs): in the first 4 weeks; non-encapsulated heterogeneous non-liquefied material
walled-off necrosis (WON or WOPN): develop after 4 weeks; encapsulated heterogeneous non-liquefied material
Clinical presentation
The walled-off collection may cause mass effect (e.g. against the biliary system, causing upstream dilatation). It may also become infected.
Pathology
WOPN consists of necrosis and subsequent liquefaction of pancreatic and/or peripancreatic tissue. It may be intrapancreatic or parapancreatic.
Radiographic features
A history of pancreatitis is necessary to exclude a complex cystic neoplasm. One should remember that an obstructing adenocarcinoma can cause pancreatitis, and if this is a concern, follow-up imaging (3-6 months) after the resolution of pancreatitis would be useful to exclude a mass.
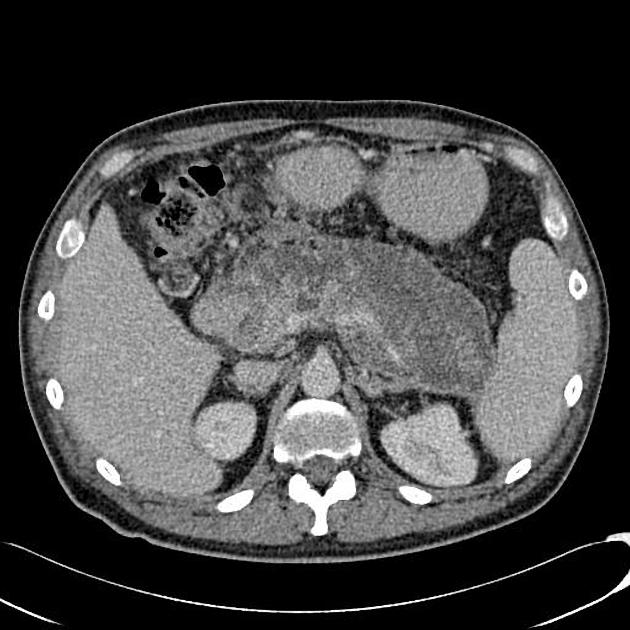
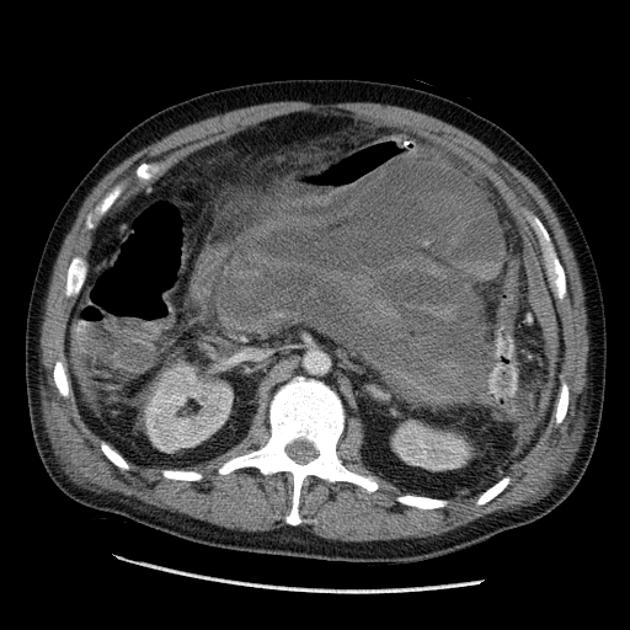
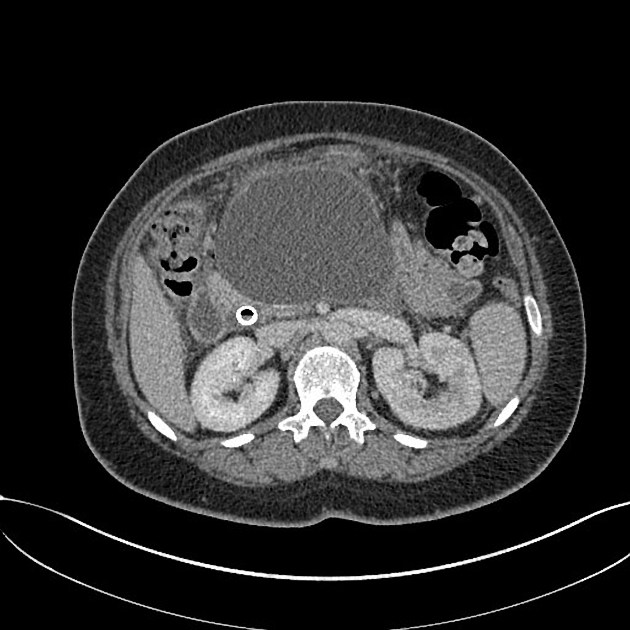
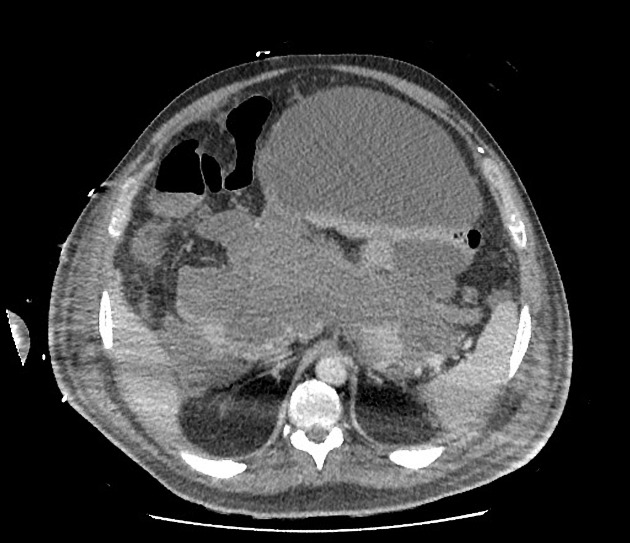
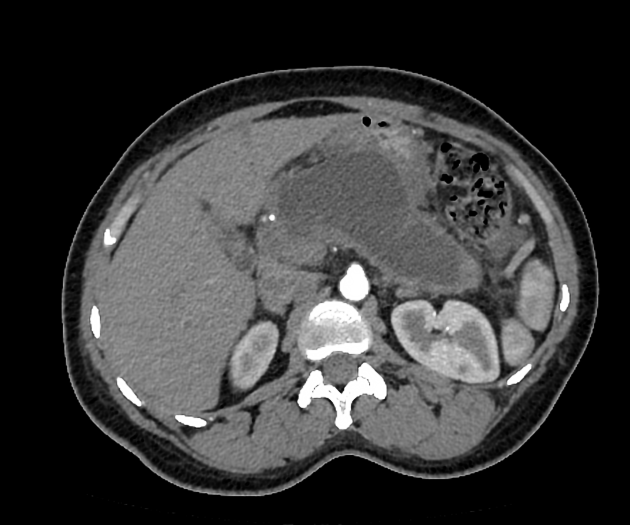
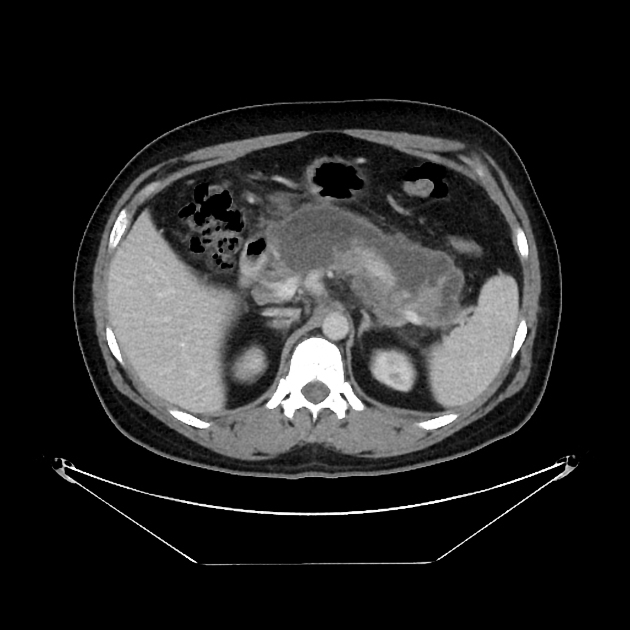
CT
cystic lesion within or around the pancreas with an area of heterogeneous attenuation non-enhancing (necrotic) tissue, surrounded by a wall 3
remember to look for other sequelae of pancreatitis (e.g. pseudoaneurysm)
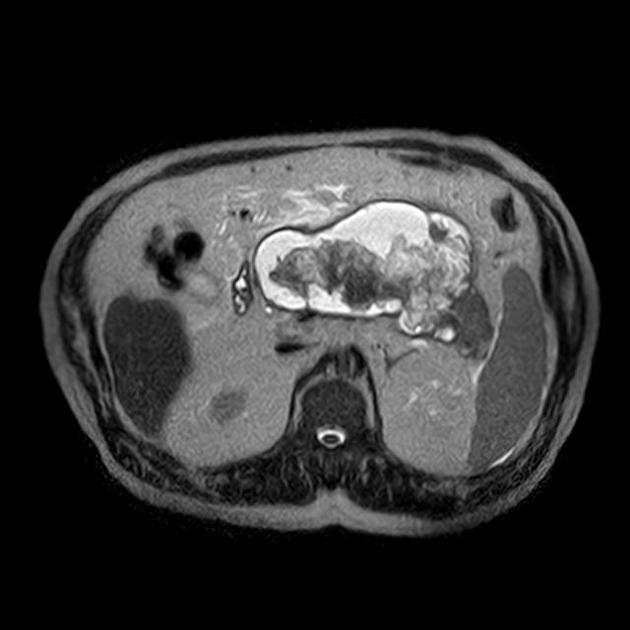
MRI
MRI is superior to CT in differentiating WOPN from pseudocyst, given its ability to depict the internal necrotic debris that favours the WOPN.
Treatment and prognosis
The mortality rate with WOPN is high but less than infected pancreatic necrosis. Management depends on the patient's symptoms and the location of the WOPN. Since 40% of walled-off pancreatic fluid collections (including pseudocysts) resolve spontaneously 4, and ~10% of patients develop complications, conservative treatment may appropriate in some asymptomatic patients 5.
Symptomatic patients should have WOPNs drained. Percutaneous catheter drainage and endoscopic retrograde cholangiopancreatography (ERCP) drainage (+/- necrosectomy) have been used to treat the walled-off necrosis. These techniques are replacing surgical drainage 1,2.
Because of the necrotic debris, WOPN usually requires a wide-bore drainage catheter as compared to the small calibre catheters that can be used to drain a pseudocyst 3.
History and etymology
The term "walled-off pancreatic necrosis" was used by Connor et al. in 2005 2.








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}