
Presentation
Abdominal distension and generalized pain. Some weight loss, but no change in bowel habit. No specific tenderness. Normal bloods and renal function.
Patient Data

Generalized paucity of bowel gas. Fat density within the right iliac fossa with possible calcification; features of a dermoid.



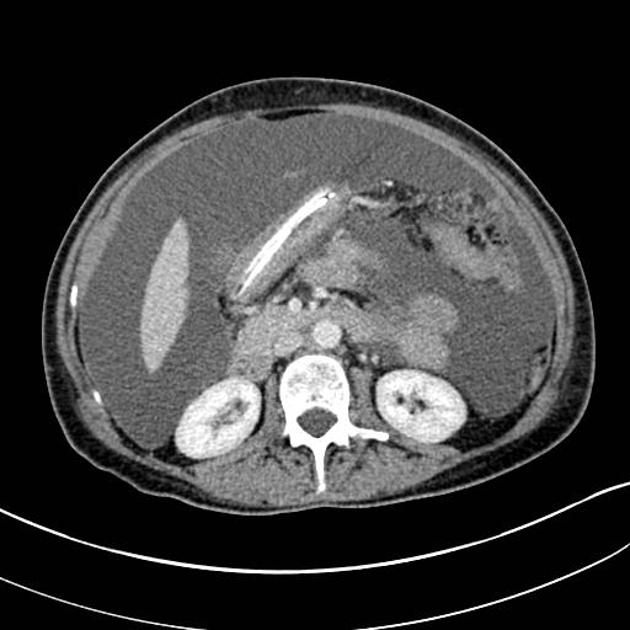
Ascites with peritoneal enhancement, omental disease and a right ovarian dermoid.
Case Discussion
The cause of the abdominal distension is shown to be ascites with peritoneal enhancement and omental disease, but no clear source. The right pelvic mass lies adjacent to the ovary and has fat, calcification and soft tissue components. Imaging findings confirm the presumed diagnosis at plain film of an ovarian dermoid.
The likely differential is primary peritoneal carcinoma, but malignant degeneration of the dermoid is on the list of differentials.
Pathology report
Needle core biopsies of fibrofatty tissue are extensively infiltrated by focally necrotic poorly differentiated carcinoma. In places, the morphology would be consistent with high grade serous carcinoma, and in keeping with primary peritoneal carcinoma. Omental biopsy high grade serous carcinoma, consistent with PPC


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.