
Presentation
Epigastric pain radiating to the back associated with two episodes of vomiting fresh blood. High D-Dimers in laboratory investigations.
Patient Data




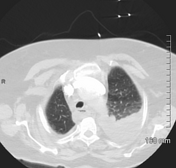


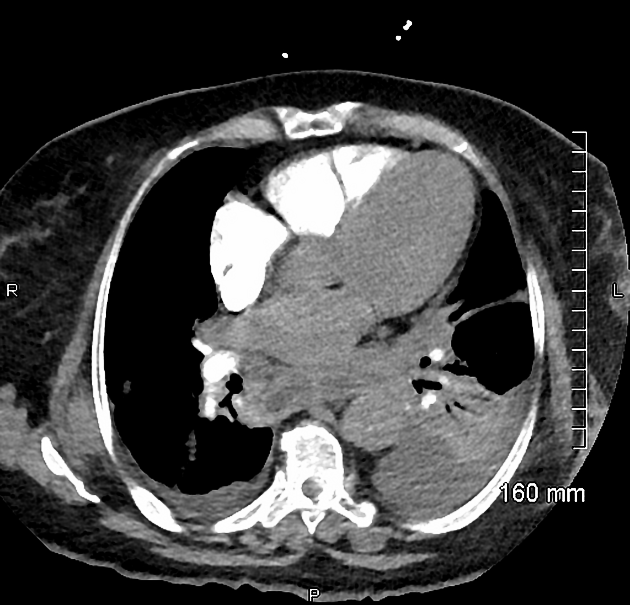
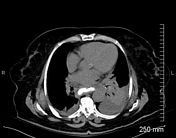
no CT evidence of major pulmonary embolism. Bilateral pleural effusions with consolidative changes in bilateral lower lobes and mild atelectatic changes in both lungs. 3 mm calcified nodule, likely an old granuloma, in the left upper lobe. No pneumothorax.
sliding hiatus hernia.
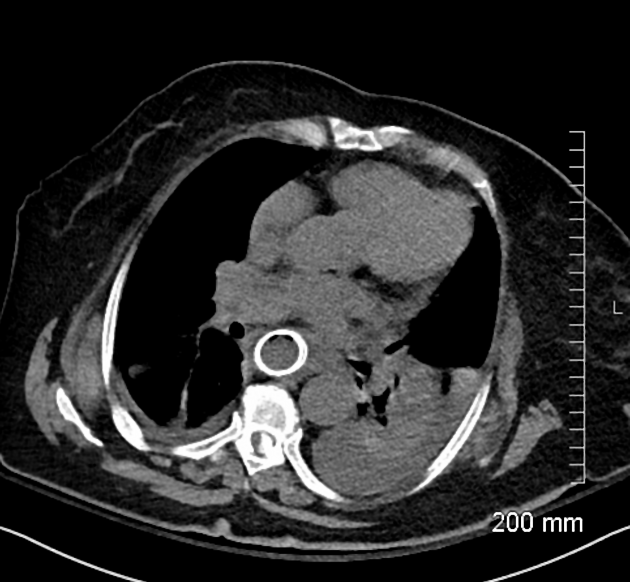
mildly dilated fluid-filled esophagus. Multiple small gas foci in the posterior mediastinum adjacent to the esophagus along with a small fluid collection behind the heart and above the left hemidiaphragm; possibility of esophageal perforation needs to be excluded and further evaluation with endoscopy or CT scan with positive oral contrast is advised.
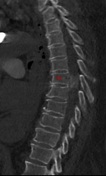
calcified lesion within the spinal canal at T6-T7 level, likely a spinal meningioma.
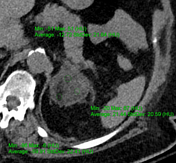
4 x 4.5 cm mixed density benign looking lesion in the left adrenal gland.
tiny peripheral/subcapsular splenic calcification.


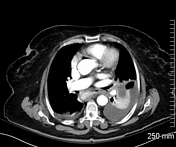



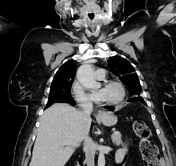



Positive oral contrast leakage from the left lateral wall of the esophagus at T6-T7 level, with extravasated oral contrast tracking/localized in to the retrocardiac fluid collection.
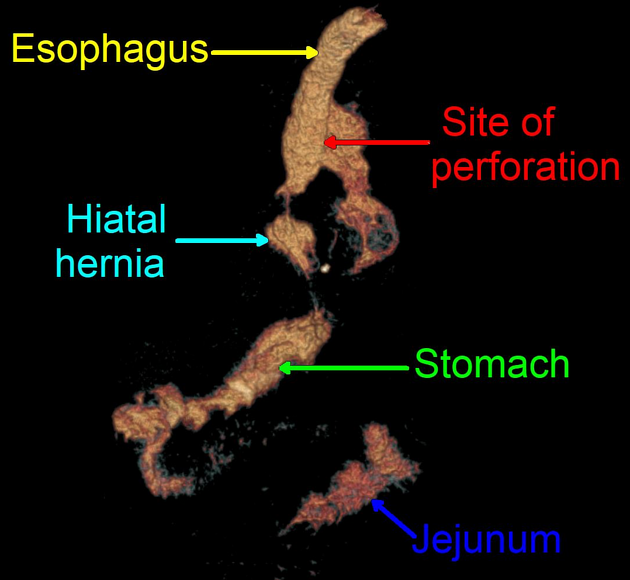
Reformatted VR image showing oral contrast opacified esophagus with site of extravasation along its left lateral wall. Oral contrast opacified hiatal hernia, stomach and jejunum are also noted.




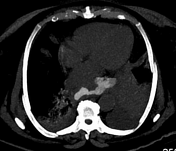
An esophageal stent is seen in place at T2-T10 level. No oral contrast extravasation is seen.
Case Discussion
The patient had tachycardia, tachypnea and desaturation (SpO2=88%). Based on these symptoms and high D-Dimers, pulmonary embolism was suspected and CT pulmonary angiogram was requested which was negative for any pulmonary embolism; however, there was a suspicion of esophageal perforation which was later confirmed with repeat CT scan with positive oral contrast, due to unavailability of endoscopy services.
Upper GI endoscopy was performed after the 2nd CT scan which showed a large defect in the esophagus at 23-24 cm from the incisor. An esophageal stent was inserted endoscopically.
The left adrenal lesion was likely an incidentaloma, as it was stable since its initial detection on a CT abdomen done five years ago. Laboratory investigations done five years ago also did not show any endocrine abnormality.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.