
Presentation
Left side chest pain with fever. Dysphagia for one week.
Patient Data

Zoomed chest X-ray PA view shows radio-opacity in the left middle and upper zones. The opacity has its broadest base peripherally in keeping with a chest wall based abnormality, in this case the pleural space.
The suggestion of an enlarged, dense, left hilum. A 'mosquito' artifact is noted along right para-spinal line.




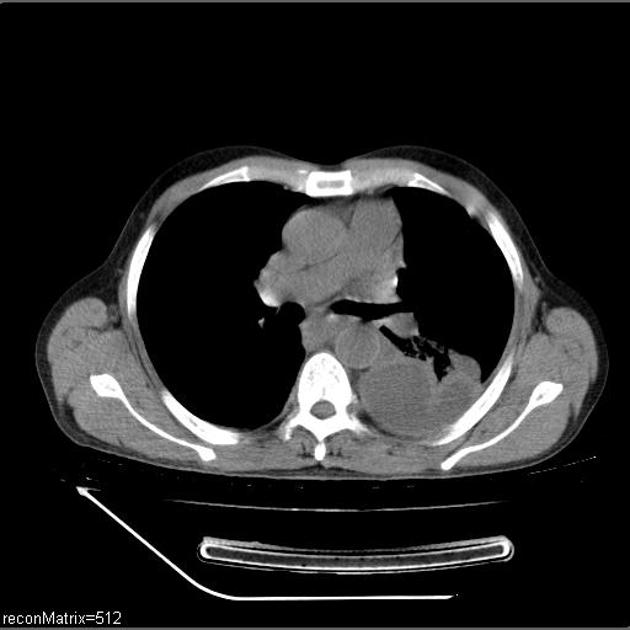
Multiloculated left sided pleural effusion with pleural thickening and enhancement. Split pleura sign is seen. There is evidence of tracking of the effusion into the posterior mediastinum with compression of the esophagus. Multiple enlarged pre-tracheal, para-tracheal and retro-aortic nodes. Ground glass opacities and fibrotic strands in the left lower lobe.

Intercostal drainage tube in-situ. Almost complete resolution of the effusion. The drained fluid was thick and yellowish.
Case Discussion
With the presenting complaints and first chest X-ray, a provisional diagnosis of thoracic empyema was made.
Subsequently the patient underwent a CT scan which showed the extent and involvement of the disease process. There was also a suspicion of an esophageal-pleural fistula on contrast enhanced images and thus subsequently an oral contrast study was performed. On oral contrast administration, there was no evidence of fistula, but it appeared as if the esophagus was thickened (endoscopy was performed which turned out to be normal).
Finally, in view of imaging findings and patient presentation, a diagnosis of thoracic empyema with mediastinitis was made and intercostal drainage performed which confirmed the presence of an infected purulent effusion.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.