
Presentation
Right middle lobe endobronchial mass - confirmed adenocarcinoma. Past history of TB. Left upper lobe subpleural lesion. Cardiothoracic surgeon queries nature of second lesion.
Patient Data
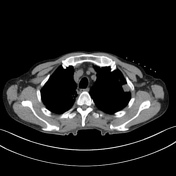


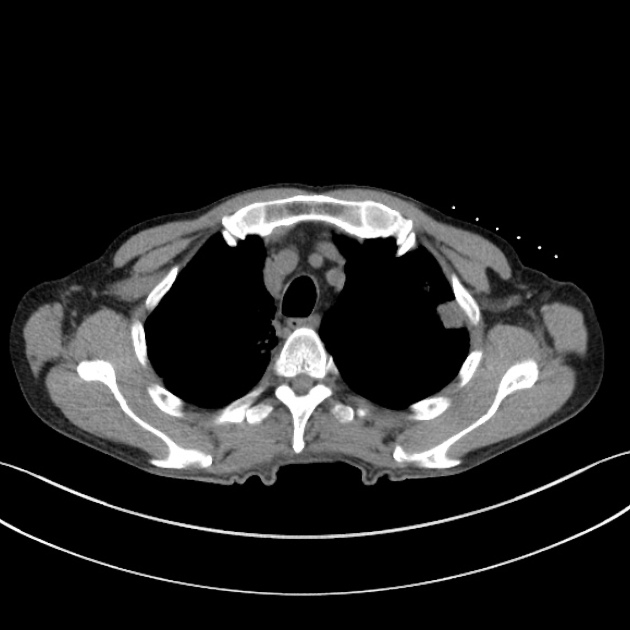
The skin surface markers have been placed over the anterior left chest - the only viable potential route for biopsy given the high location of the lesion.
The scapula is obstructive posteriorly and the subclavian vessels and ribs laterally.
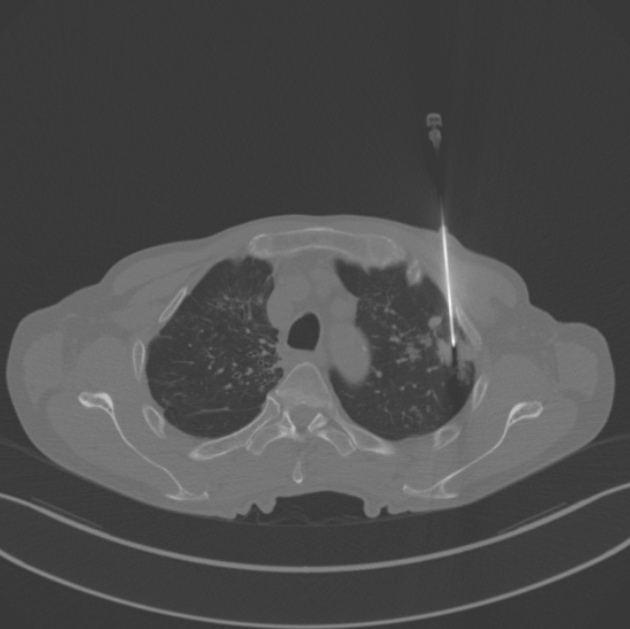
The CT fluroscopy data is present in one cycle from the procedure - acquired using 'i-spiral' technique.
The initial infiltration needle, co-axial needle siting, subsequent advancement before biopsy acquisition and post biopsy check for pneumothorax are shown.

A pneumothorax is evident on a CXR performed the following morning - the most common complication of a lung biopsy.
Initial conservative management.
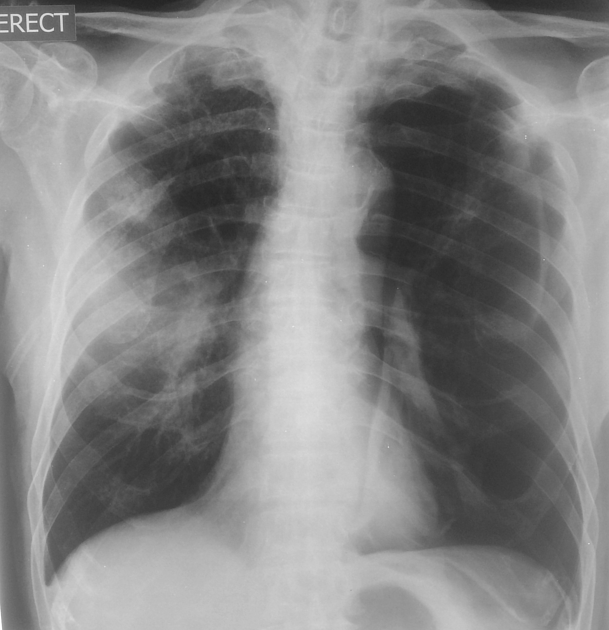
24 hours later the pneumothoarax was significantly larger.
A pleural drain was inserted.
Case Discussion
Modern CT machines with a 32 slice and above capability offer CT fluroscopic functions for use in CT guided procedures.
This has several advantages:
a. More control to operating radiologist
b. Speedier procedure
c. Lower dose procedure
Initial systems allowed for a single slice to be shown - this had its limitations. However, one can now acquire 3 images (head, center, feet) given much more confidence on the exact needle position.
The process of biopsy remains otherwise the same, with a flawless biopsy ( no repositioning due to angulation of patient movement ) having 5 steps.
A. Image aqusition with markers to plan approach.
B. Check of maintained position and angulation planning with infiltration needle.
C. Co-axial insertion - check correct route prior to pleural breech.
D. Advancement of co-axial needle to lesion and biopsy aqusition.
E. Post biopsy pneumothorax check.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.