
Presentation
Right iliac fossa pain
Patient Data



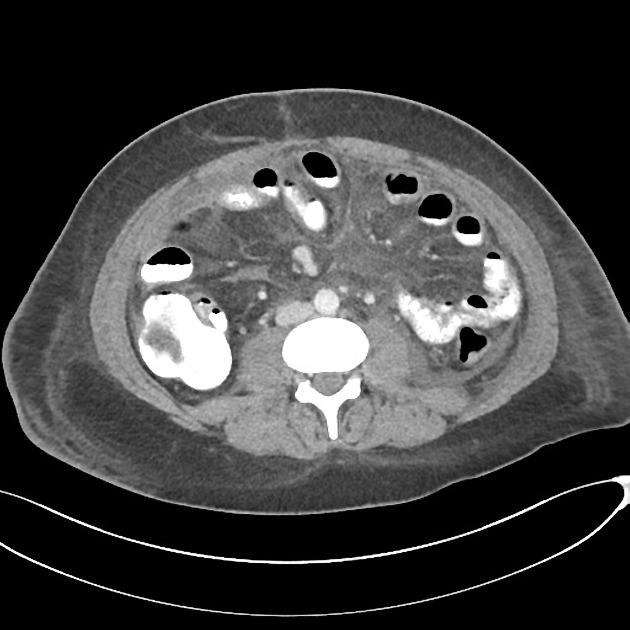
Large ileocolic collection containing fluid and gas in the right iliac fossa, abutting the inflamed terminal ileum. It has a well-defined wall with thickening and enhancement and measures 10.6 x 6.8 x 8.7 cm, displacing the inflamed ileum superiorly and posteriorly. The anterior and lateral borders abut the abdominal wall, with no intervening bowel loop suggesting percutaneous drainage would be feasible.
Multiple smaller collections with enhancing walls:
- on the medial aspect of the inflamed terminal ileum, an adjacent collection measures 1.6 x 2.7 cm.
- semilunar shaped right pelvic collection measures 4.2 x 2.3 cm and appears to communicate with the larger right iliac fossa collection more superiorly.
- a small left iliac fossa collection anterior to the external iliac vessels measuring 2.0 x 2.8 cm. Adjacent sigmoid colonic bowel thickening suggests either reactive colitis or an inflammatory skip lesion.
No bowel dilatation.
Retroperitoneal edema and fat stranding is noted, particularly surrounding the psoas muscles. Small amount of intraperitoneal fluid surrounding the liver and spleen. Cholelithiasis. No sacroilitis.
Case Discussion
This patient had been diagnosed with Crohn disease 2 years prior and had been slowly non-compliant with meds in the preceeding 2 months before this presentation.
After 6 weeks in hospital treated with IV ABs and multiple image-guided percutaneous collection drainages, the patient recovered and was discharged.
IBD has an increased risk of gallstones.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.