
Presentation
Metastatic breast cancer; yellow fluid being aspirated from implanted venous catheter.
Patient Data


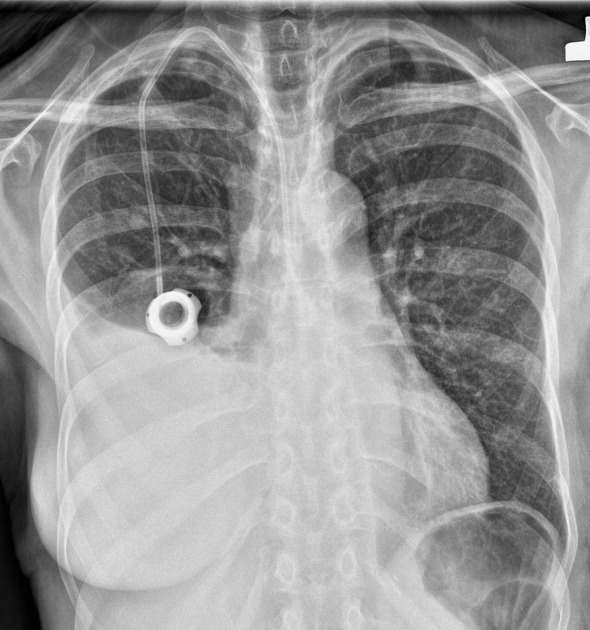
Large right pleural effusion, likely malignant in nature, patient will likely benefit from thoracentesis and drainage catheter placement.
Bilateral multiple metastatic lung nodules.
With the above history, a radiologist should think out of the box for the rare complications following implanted venous catheter placement. Recommend a fluoroscopic study for evaluation of the tip of the implanted venous catheter as the tip on lateral view suggests it has an extrapleural course or it has perforated the SVC and has passed out into the mediastinum.
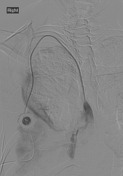
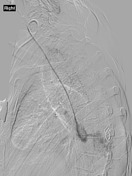

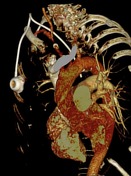
The catheter of the right chest port has an extravascular course for its entire length and the tip of the catheter terminates in the mediastinum/pleural space. The contrast flows into the posterior right pleural space.





A right chest wall port has been placed. Neither the catheter nor catheter tip is intravascular and terminates along the posterior medial aspect of the right thorax. There was a new development of a large fluid collection within the right hemithorax, which may represent a large right infusothorax from chemotherapy.
Case Discussion
The implanted venous catheter was placed under fluoroscopic guidance by surgeons; no static image was obtained postoperatively.
The patient received chemotherapy via this port for 8 weeks. Despite its inadvertent malposition, there has been a good response to chemotherapy for breast cancer.
Following the chest x-ray, fluoroscopy confirmed the extravascular pleural course of implanted venous catheter, which was confirmed on CT. The next day, a VATS was performed and the port was removed; the pleural effusion was not bloody. At that time it was confirmed that the port was in the pleural space all along and the chemotherapy was absorbed by the pleural membrane into the bloodstream effectively.
Important lesson: It is very important to ensure ports are intravascular by aspirating blood before infusing drugs.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.