
Presentation
Cough for six months. Non-resolving opacity on chest x-ray.
Patient Data

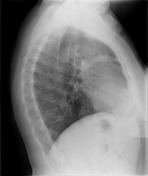
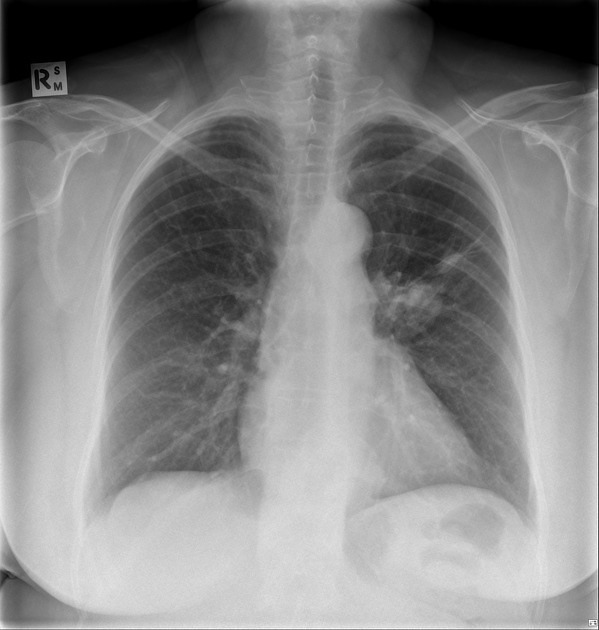
Rounded left hilar opacity with branching opacity anteriorly on the lateral projection.







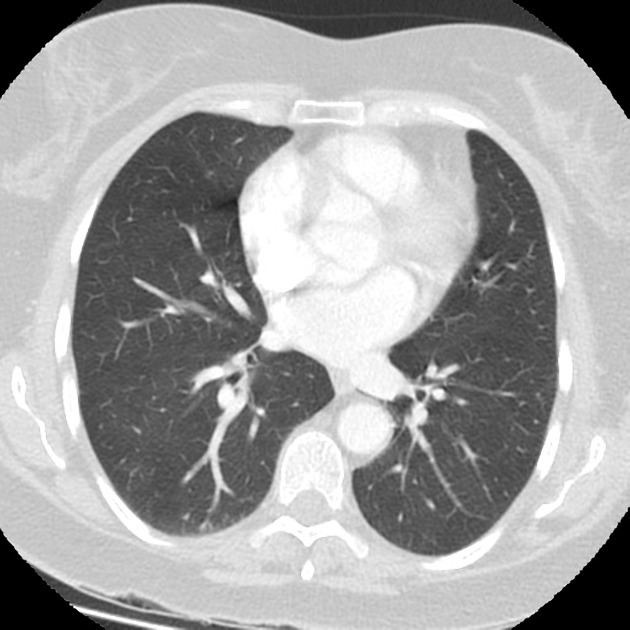
Branching low-density opacities in the left upper lobe extending from the hilum. Small mass at the superior aspect of the left hilum. No lymphadenopathy.

MACROSCOPIC DESCRIPTION:
Left upper lobe": A lung lobe 185x110x55mm with bronchovascular remnants up to 25mm. Arising in the hilum and involving the bronchus is a rubbery tan-pink tumor 21x20x19mm. The tumor is 6mm from the bronchovascular margins and 3mm from the hilar margin. 26mm from the tumor and 1mm from the pleura there is a firm white nodule 6mm. Peripheral to the tumor is an area where the lung shows dilated bronchi up to 12mm in diameter which lie 2mm from the pleura.
MICROSCOPIC DESCRIPTION:
Sections of the lung show a well-demarcated moderately cellular tumor, which invades into a bronchus. The tumor forms cohesive nests, cords and rosettes, surrounded by vascularized stroma. The tumor cells have mildly enlarged round nuclei, granular chromatin, inconspicuous nucleoli and moderate amounts of granular eosinophilic cytoplasm. 1 mitosis per 10 high power field is seen. There is no evidence of necrosis. The visceral pleura is uninvolved. No evidence of lymphovascular invasion is seen. The tumor is completely excised. The bronchial and vascular margins are clear. The tumor is pushing into a hilar lymph node with direct involvement for 3mm. Another benign hilar lymph node is present. The subpleural nodule is a pulmonary hamartoma. There is elongated respiratory type epithelium, being surrounded by nodules of cartilage and myxomatous stroma. The remaining lung parenchyma show a few dilated bronchi but they are not inflamed. The tumor cells are synaptophysin and CD56 positive. The Ki-67 index is about 2%.
COMMENT:
The features are those of typical carcinoid.
Courtesy: Pathology Department, The Royal Melbourne Hospital.
Case Discussion
The low-density branching opacities are typical for bronchoceles, and when seen a careful search should be made for an obstructing lesion, of which carcinoids are a typical culprit.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.